Techniques of Cognitive Therapy
Audiologist-delivered CBT is focused on managing tinnitus/hyperacusis/misophonia-related distress (Aazh & Allott 2016; Aazh & Moore 2018b; Aazh & Moore 2018a). Patients with symptoms of other psychological disorders should be referred to mental health professionals for assessment and appropriate management of their symptoms at the same time or prior to their tinnitus and hyperacusis rehabilitation.
The audiologist-delivered CBT for tinnitus and/or hyperacusis involves individual face-to-face sessions, each lasting about one hour. Table below shows a summary of the typical techniques used in each session. For details see Dr. Aazh’s paper on
audiologist-delivered CBT for tinnitus and/or hyperacusis published in International Journal of Audiology.
Summary of the interventions provided in each audiologist-delivered cognitive behavioural therapy (CBT) session for management of tinnitus and/or hyperacusis.
| Session 1 |
Exploration of tinnitus/hyperacusis-related distress using in-depth interview
Evaluation of the patient’s cognitive, behavioural and emotional reactions to tinnitus/sound and the impact these have on their life.
Development of a cognitive behavioural formulation for tinnitus/hyperacusis distress
Enhancement of the patient’s motivation for the therapy
Offer of full CBT or discharge |
| Session 2 |
Design of a behavioural experiment (BE) to target and challenge troublesome thoughts
Patient to complete the BE as a between-session assignment |
| Session 3 |
Reviewing and reflecting on the outcomes of the BE
Creation of counter-statements to negative thoughts
Issuing the diary of thoughts and feelings (DTF) to be filled in as a between-session assignment |
| Session 4 |
Reviewing of the DTF and giving help to the patient to appraise and modify the thoughts responsible for producing tinnitus/hyperacusis-related distress
Issuing another DTF to be filled in as a between-session assignment |
| Session 5 |
Reviewing of the DTF
Developing “acceptance” of tinnitus/hyperacusis
Further education about CBT |
| Session 6 |
Reviewing and reflecting on progress
Discharge |
Case formulation
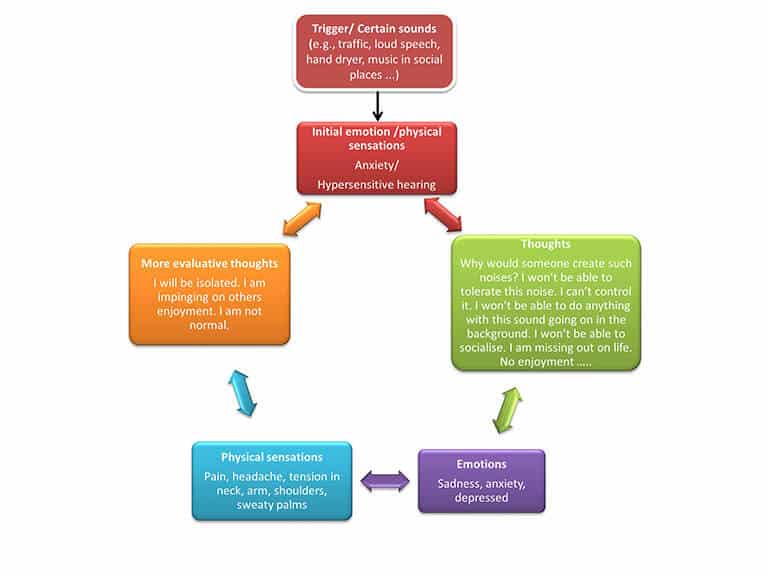
In-depth interview is used in order to explore the impact of tinnitus and/or hyperacusis/misophonia on the patient’s life. If the tinnitus and/or hyperacusis does adversely affect the patient’s activities or mood then the therapist should help the patient to explore their thoughts, emotional reactions, physical sensations, and safety-seeking behaviours. The information gathered here will be used for formulation of the processes and stages involved in producing their tinnitus and/or hyperacusis-related distress (Muran 1991). The formulation will be shared with patients and the principles of CBT will be discussed. Examples of formulation for tinnitus and hyperacusis are shown in Figures 1 and 2. The case formulations for tinnitus and hyperacusis which are proposed here begin with the initial emotional response and physical sensations related to the experience of tinnitus or hyperacusis. These initial symptoms are then followed by the individuals’ negative thoughts leading to further negative emotions, physical sensations, and evaluative thoughts which feed back into the patient’s initial reaction leading to exacerbation of their symptoms, a vicious cycle.
Behavioural experiment
Behavioural experiment (Bennett-Levy et al. 2004) should be used in order to help the patient to explore their negative predictions about what might happen to them when exposed to sounds that they found unpleasant (in the case of hyperacusis/misophonia) or when they become aware of their tinnitus, and the precautions that they typically take to prevent these from happening (Bennett-Levy et al. 2004; McManus et al. 2012). The behavioural experiment provides an opportunity for the patient to drop these precautions or safety seeking behaviours so that they could face their fear, which is intended to help them to find out whether their negative predictions and fear are justified. Most patients state that at least some of their predictions do not come true.
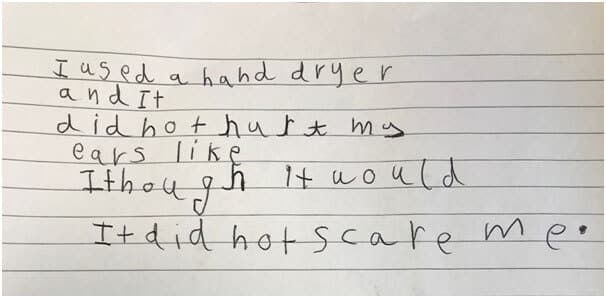
For example a 6 years old girl with hyperacusis found the classroom environment difficult due to noise levels and at times had to cover her ears. This created unnecessary stress which hampered her progress in school and impacted her self-confidence. Her mum reported that when they went to a theme park she covered her ears for almost the whole time. During the therapy she learned how to explore her thoughts and modify them. After a behavioural experiment she wrote the text below which showed her progress in resolving her intolerance to sound.
Then patients are encouraged to create counter-statements for their negative thoughts based on the evidence they gathered during the experiment (Henry & Wilson 1995). Patients are encouraged to use these counterstatements in real-life scenarios as soon as the troublesome tinnitus and/or sound-related thoughts goes through their mind.
Diary of Thoughts and Feelings (DTF)
DTF is used to provide a structured method for the patient to take notes about their tinnitus and/or sound-related problems, and their associated thoughts and emotions (Bennett-Levy 2003; McManus et al. 2012). DTF is completed by patients between sessions. During the session, audiologist encourages the patient to think of the advantages and disadvantages of the thoughts that they recorded in the DTF, and to replace them by counter-statements if the patient decide that their thoughts were unrealistic or unhelpful. The overall approach is collaborative with a strong emphasis on the clinician and patient exploring the problem together. In the other words, patient makes discoveries with the help of careful questioning from the audiologist rather than the audiologist giving information and advice.
References
Aazh, H., & Allott, R. (2016). Cognitive behavioural therapy in management of hyperacusis: a narrative review and clinical implementation.
Auditory and Vestibular Research,
25, 63-74.
Aazh, H., & Moore, B. C. J. (2018a). Effectiveness of audiologist-delivered cognitive behavioral therapy for tinnitus and hyperacusis rehabilitation: outcomes for patients treated in routine practice
American Journal of Audiolgy,
[Epub ahead of print], 1-12.
Aazh, H., & Moore, B. C. J. (2018b). Proportion and characteristics of patients who were offered, enrolled in and completed audiologist-delivered cognitive behavioural therapy for tinnitus and hyperacusis rehabilitation in a specialist UK clinic.
Int J Audiol,
57, 415-425.
Bennett-Levy, J. (2003). Mechanisms of change in cognitive therapy: the case of automatic thought records and behavioural experiments
Behavioural and Cognitive Psychotherapy,
31, 261-277.
Bennett-Levy, J., Butler, G., Fennell, M., et al. (2004).
Oxford guide to behavioural experiments in cognitive therapy. Oxford, UK Oxford University Press.
Henry, J., & Wilson, P. (1995). The psychological management of tinnitus: comparison of a combined cognitive educational program, education alone and a waiting-list control.
The international tinnitus journal,
2, 9-20.
McManus, F., Van Doorn, K., & Viend, J. (2012). Examining the effects of thought records and behavioural experiments in instigating belief change.
Journal of Behaviour Therapy and Experimental Psychiatry,
43, 540-548.
Muran, J. C. (1991). A reformulation of the ABC model in cognitive psychotherapies: implications for assessment and treatment.
Clin Psychol Rev,
11, 399-418.