A Thirteen Years Old Boy With Severe Misophonia: Treatment Outcome and Mum’s Reflections.
Background
We use a pseudo name Jack. Jack was diagnosed with severe misophonia with a significant hyperacusis component
1,2. He was under the care of a child and adolescent psychiatrist for OCD and anxiety. His trigger noises were mum’s voice, whistles and shrill letter “S” or other consonants only when mum spoke, burping, swallowing, chewing, and clicking sounds. His emotional reactions were anger, anxiety and disgust. He also presented with psychical sensations of distorted hearing and pain in ears when hearing certain trigger sounds. His behavioural reactions ranged from avoidance, mimicry, asking people to say things right, or to say sorry, and violence at time.
Therapy and outcome
Following the initial assessment, he received 20 sessions of specialist rehabilitative programme on misophonia and hyperacusis management based on cognitive behavioural therapy (CBT) approach
3-7. At the beginning of the therapy, he could not sit with his mum in the same room due to the trigger sounds she made. Therefore, I had to split the sessions so I can work with Jack on his own followed by giving a brief to his mother at the end of each session. Jack was very motivated and his parents were very supportive throughout the therapy programme. The change in effect of his misophonia and hyperacusis on his life as measured via Misophonia Impact Questionnaire (MIQ/parent), Hyperacusis Impact Questionnaire (HIQ/parent), overall sensitivity to sound as measured via Sound Sensitivity Symptoms Questionnaire (SSSQ/parent) and the score on Screening for Anxiety and Depression (SAD/parent), are shown in the graph below:
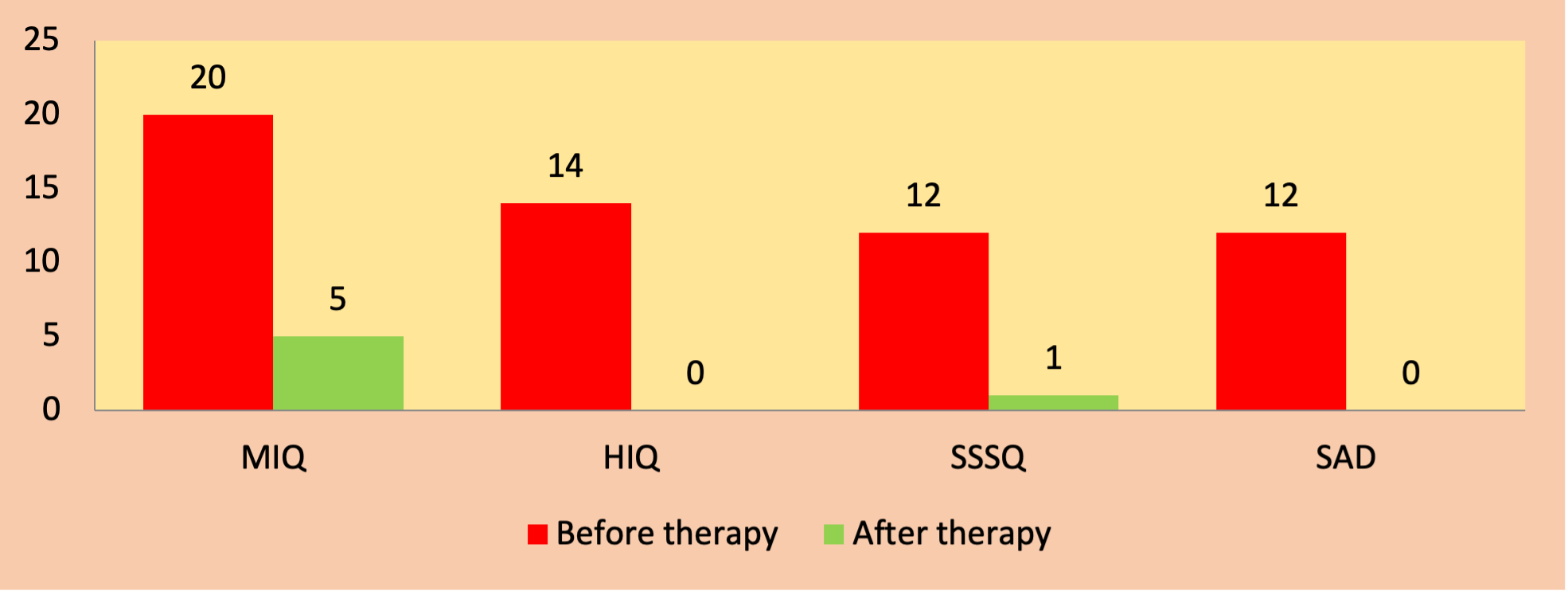
As shown in the graph Jack shown considerable improvements in his ability to manage his misophonia and general sensitivity to sound. His post-therapy scores on all 4 questionnaires shown above were within the normal range.
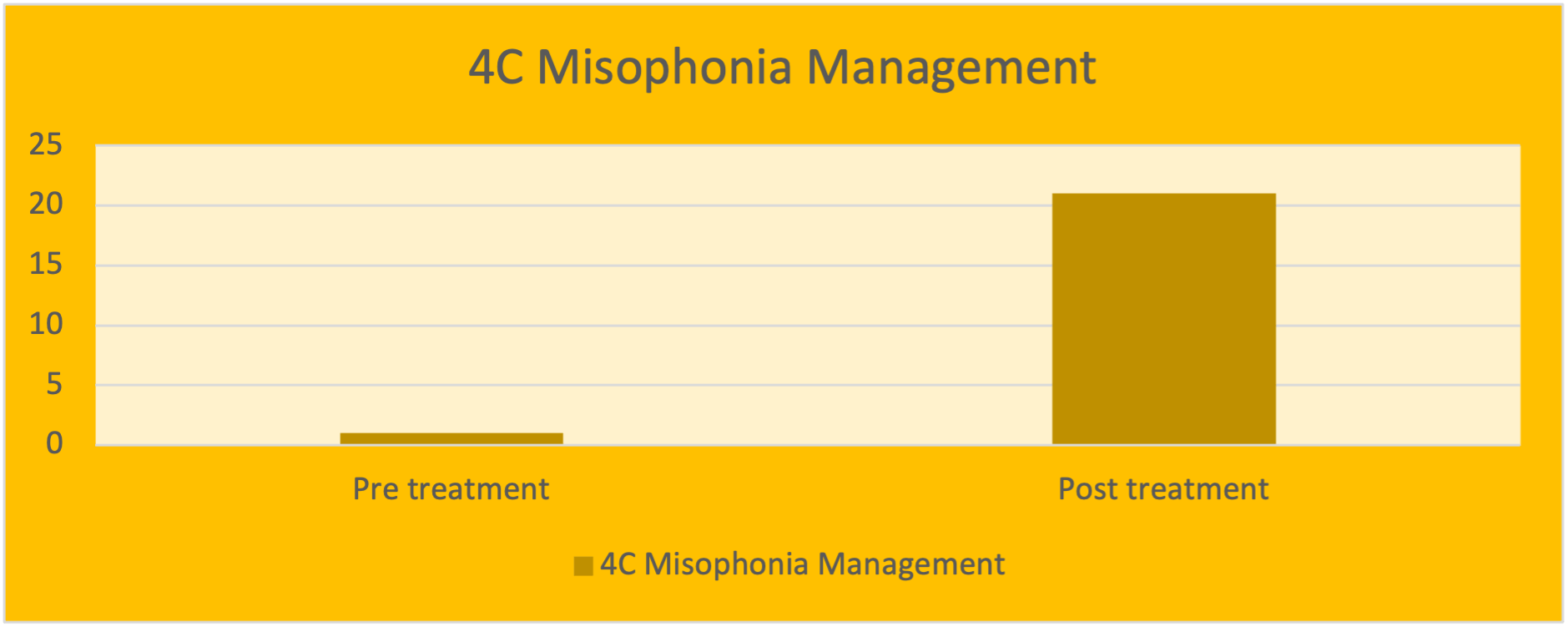
As illustrated in the graph below his score on 4C Misophonia Management Questionnaire improved from 0% (before treatment) to 21% (after treatment). The lowest possible score is 0% which means not confident at all in managing misophonia. The highest possible score is 100% which means confident in managing this condition.
Conclusion
Jack has complied with the treatments provided and made considerable improvement in managing his misophonia. It is highly likely that by the passage of time, if he consistently applies the CBT knowledge gained throughout the therapy, he will be able to master the CBT skills and fully minimise the effect of misophonia on his life. We agreed that no further therapy is necessary at this stage and I have discharged him from my care.
Feedback from mum
Working with Dr Hashir Aazh has been a positive and life changing experience for our son and family. Misophonia can be such a poorly understood and under researched area, and we were struggling with the impact it was having on our son’s wellbeing as well as our whole family. After trying counselling with a local therapist and waiting for over a year at CAMHS- with no guarantee of then having a therapist who would then understand misophonia- we found Hashir and after an initial consultation the relief of talking to someone who understood and felt they could help us was huge.
Dr Hashir took the time to really get to know our son, and it became apparent even after the first couple of sessions, that things were starting to ‘get into’ our son’s mindset and change how he was feeling and thinking about his misophonia, but more than that how he saw himself. Working remotely on Zoom/Skype really suited us, and throughout the process it felt as if Hashir really took the time to adapt his practice around us (my son could not tolerate being in the same room as me), building in gaps and stepping back slightly where it was appropriate, or conversely building momentum when things were going well with targeted tasks and sessions closer together. It took a while but working together things are very different now. Our son will continue to live with misophonia, but he understands it now, likes himself again and most importantly knows how to live happily in our family.
References
- Aazh H, Moore BCJ. Prevalence and characteristics of patients with severe hyperacusis among patients seen in a tinnitus and hyperacusis clinic Journal of American Academy of Audiology 2018;29:626-633.
- Danesh A, Aazh H. Misophonia: A Neurologic, Psychologic, and Audiologic Complex. The Hearing Journal 2020;23:20-23.
- Aazh H, Allott R. Cognitive behavioural therapy in management of hyperacusis: a narrative review and clinical implementation. Auditory and Vestibular Research 2016;25:63-74.
- Aazh H, Bryant C, Moore BCJ. Patients’ perspectives about the acceptability and effectiveness of audiologist-delivered cognitive behavioral therapy for tinnitus and/or hyperacusis rehabilitation. American Journal of Audiology 2020;28:973-985.
- Aazh H, Landgrebe M, Danesh A et al. Cognitive behavioral therapy for alleviating the distress caused by tinnitus, hyperacusis and misophonia: Current perspectives. Psychology Research and Behavior Management 2019;23:991-1002.
- Aazh H, Moore BCJ. Proportion and characteristics of patients who were offered, enrolled in and completed audiologist-delivered cognitive behavioural therapy for tinnitus and hyperacusis rehabilitation in a specialist UK clinic. International Journal of Audiology 2018;57:415-425.
- Aazh H, Moore BCJ. Effectiveness of audiologist-delivered cognitive behavioral therapy for tinnitus and hyperacusis rehabilitation: outcomes for patients treated in routine practice American Journal of Audiology 2018;27:547-558.