Tinnitus is perception of sound in the ears or head with no acoustic stimulation. People often describe their tinnitus as buzzing noise in the ears or head, high-pitched noise, hissing noise, whistle, waterfall and grinding wheel, ringing, white noise, wind noise, bubbles and clicks, beep, and humming noise. About 20% of patients are unable to describe what their tinnitus sounds like. Hyperacusis is intolerance to certain everyday sounds that causes significant distress and impairment in social, occupational, recreational, and other day-to-day activities.
Tinnitus and hyperacusis are associated with depression. Exploring the factors predicting depression in patients with tinnitus/ hyperacusis/ misophonia is important as it can guide psychiatric management of the co-morbid depression in this population. Dr. Aazh’s tinnitus team developed the first mathematical model] which explained over 60% of the variance of depression severity in over 600 patients with tinnitus and/or hyperacusis.
Dr. Aazh’s tinnitus team used mediation analysis to assess the direct and indirect effects of tinnitus loudness on the depression score. In addition, they assessed the direct and indirect effects of reduced uncomfortable loudness levels (ULLs), which is a measure for hyperacusis, on the depression score.
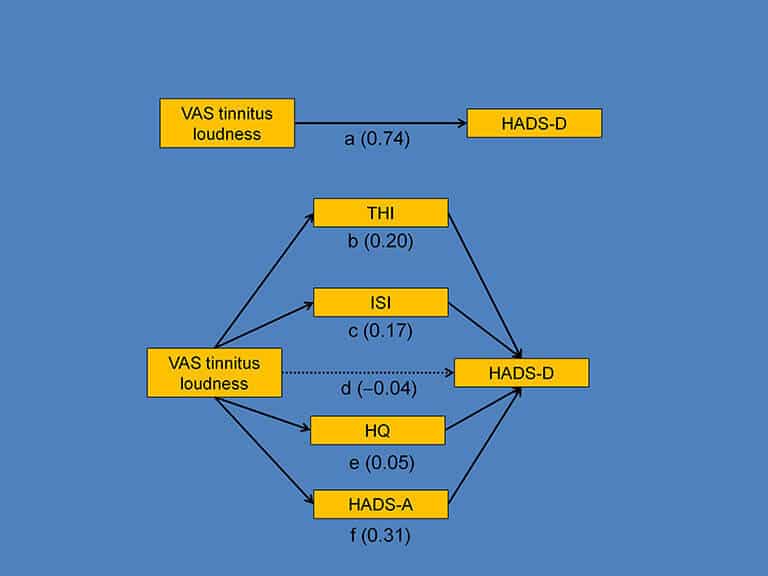
Mathematical model explaining the underlying mechanism that relate tinnitus loudness and depression
Regression analysis showed a statistically significant relationship between tinnitus loudness and depression (path “a”). Mediation analysis showed that the indirect effects of tinnitus loudness on depression via tinnitus handicap (path “b”), via insomnia (path “c”), via hyperacusis (path “e”), and via anxiety (path “f”). The total indirect effect was significant. The direct effect of tinnitus loudness on depression (path “d”) was not statistically significant. In summary, the relationship between tinnitus loudness and depression was fully mediated via tinnitus handicap, insomnia, hyperacusis, and anxiety.
This is consistent with the idea that high tinnitus loudness is associated with tinnitus handicap, hyperacusis handicap, anxiety, and insomnia, and these in turn lead to depression. The clinical implication for audiologists is that for patients who suffer from tinnitus, depressive symptoms may be alleviated if tinnitus-induced anxiety, tinnitus handicap and hyperacusis are managed adequately, even if the self-perceived tinnitus loudness remains unchanged. Past research has shown that although tinnitus loudness is only minimally reduced following various forms of tinnitus rehabilitation, effect of tinnitus on patient’s life, tinnitus handicap, typically improve. This improvement may be sufficient to reduce the severity of depression.
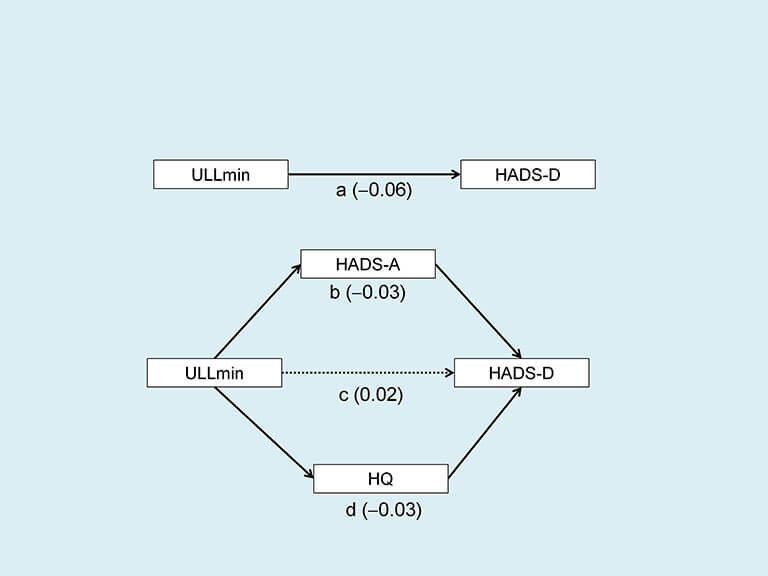
Mathematical model explaining the underlying mechanism that relates hyperacusis and depression
Linear regression analysis showed a small but statistically significant negative relationship between the Uncomfortable Loudness Levels (ULLs) and depression (path “a”). Mediation analysis showed the indirect effects of ULLs on depression via anxiety (path “b”), and via hyperacusis handicap (path “d”). The total indirect effect was significant. The direct effect of the ULL on depression (path “c”) was not statistically significant. In summary, the relationship between ULL and depression was fully mediated via hyperacusis handicap and anxiety.
Although it has been reported that people with hyperacusis often have lower than normal ULLs in one or both ears and 42-47% of them may also suffer from depression, the mechanism that produces depression in patients with hyperacusis does not seem to be explained by reduced ULLs. Therefore, future research should focus on factors that might lead to depression in patients with hyperacusis.
 Dr. Aazh’s tinnitus team used mediation analysis to assess the direct and indirect effects of tinnitus loudness on the depression score. In addition, they assessed the direct and indirect effects of reduced uncomfortable loudness levels (ULLs), which is a measure for hyperacusis, on the depression score.
Dr. Aazh’s tinnitus team used mediation analysis to assess the direct and indirect effects of tinnitus loudness on the depression score. In addition, they assessed the direct and indirect effects of reduced uncomfortable loudness levels (ULLs), which is a measure for hyperacusis, on the depression score.
 This is consistent with the idea that high tinnitus loudness is associated with tinnitus handicap, hyperacusis handicap, anxiety, and insomnia, and these in turn lead to depression. The clinical implication for audiologists is that for patients who suffer from tinnitus, depressive symptoms may be alleviated if tinnitus-induced anxiety, tinnitus handicap and hyperacusis are managed adequately, even if the self-perceived tinnitus loudness remains unchanged. Past research has shown that although tinnitus loudness is only minimally reduced following various forms of tinnitus rehabilitation, effect of tinnitus on patient’s life, tinnitus handicap, typically improve. This improvement may be sufficient to reduce the severity of depression.
This is consistent with the idea that high tinnitus loudness is associated with tinnitus handicap, hyperacusis handicap, anxiety, and insomnia, and these in turn lead to depression. The clinical implication for audiologists is that for patients who suffer from tinnitus, depressive symptoms may be alleviated if tinnitus-induced anxiety, tinnitus handicap and hyperacusis are managed adequately, even if the self-perceived tinnitus loudness remains unchanged. Past research has shown that although tinnitus loudness is only minimally reduced following various forms of tinnitus rehabilitation, effect of tinnitus on patient’s life, tinnitus handicap, typically improve. This improvement may be sufficient to reduce the severity of depression.
 Although it has been reported that people with hyperacusis often have lower than normal ULLs in one or both ears and 42-47% of them may also suffer from depression, the mechanism that produces depression in patients with hyperacusis does not seem to be explained by reduced ULLs. Therefore, future research should focus on factors that might lead to depression in patients with hyperacusis.
Although it has been reported that people with hyperacusis often have lower than normal ULLs in one or both ears and 42-47% of them may also suffer from depression, the mechanism that produces depression in patients with hyperacusis does not seem to be explained by reduced ULLs. Therefore, future research should focus on factors that might lead to depression in patients with hyperacusis. 







