Hyperacusis is the perception of certain everyday sounds, such as domestic noise or noise in public places (e.g., loud music, sirens, motorcycles, building work, lawn mower, people shouting or speaking loudly, hand dryers in public toilets, hair dryers, kitchen appliances etc) as too loud or painful in such a way that it causes significant distress and impairment in social, occupational, recreational, and other day-to-day activities. In addition to the experience of discomfort when hearing certain loud sounds, individuals with hyperacusis often report physical symptoms such as headaches, balance problems, dysosmia (distortion of smells), and light sensitivity.
Individuals with hyperacusis can also get disturbed by general environmental noise (e.g., noise in the neighbourhood, nearby airports and industrial facilities, distant traffic sound, noisy pipes or cracking noises in the house, air conditioning, etc). This is a sign of high level of noise sensitivity which is a personality trait that can coexist with hyperacusis.

Individuals with hyperacusis perceive certain everyday sounds as too loud, uncomfortable, or painful in such a way that it causes significant distress and impairment in their day-to-day life. In addition, they may experience high level of noise sensitivity which makes it hard for them to cope with general environmental noise.
Human hearing system has three sections, the outer ear, middle ear, and inner ear, as illustrated in Figure 2. Sound waves are collected via Auricle and travel down the external auditory meatus where they cause the Tympanic membrane (eardrum) to vibrate. The vibrations of the Tympanic membrane are transferred through the middle ear’s ossicles to the cochlea in the inner ear. Inside the cochlea there are specialised sensory cells called hair cells. These are responsible for detecting vibrations in the cochlea and stimulating the cochlear nerve. The electrical signals in the cochlear nerve are sent through various processing centres to the part of the brain that analyses sound, where they are perceived as sound. The cochlear nerve and the hearing parts of the brain control how loud we should hear sounds. For people with hyperacusis, these parts of the brain go out of calibration and tend to over-amplify certain sounds. In other words, a person with hyperacusis hear certain sounds louder than normal. This doesn’t mean that they are at higher risk of a hearing damage from the noises compared to other people. It means that they perceive sounds much louder than others hence it can be very disturbing and disabling for some. The anxiety caused by the experience of hyperacusis stops the brain to automatically re-adjust itself. Therefore, the treatment for hyperacusis is to reduce the anxiety induced by perception of the loud noises in order to give the brain an opportunity to recalibrate itself over time. Later in this page you will learn about how cognitive behavioural therapy (CBT) can help with hyperacusis.
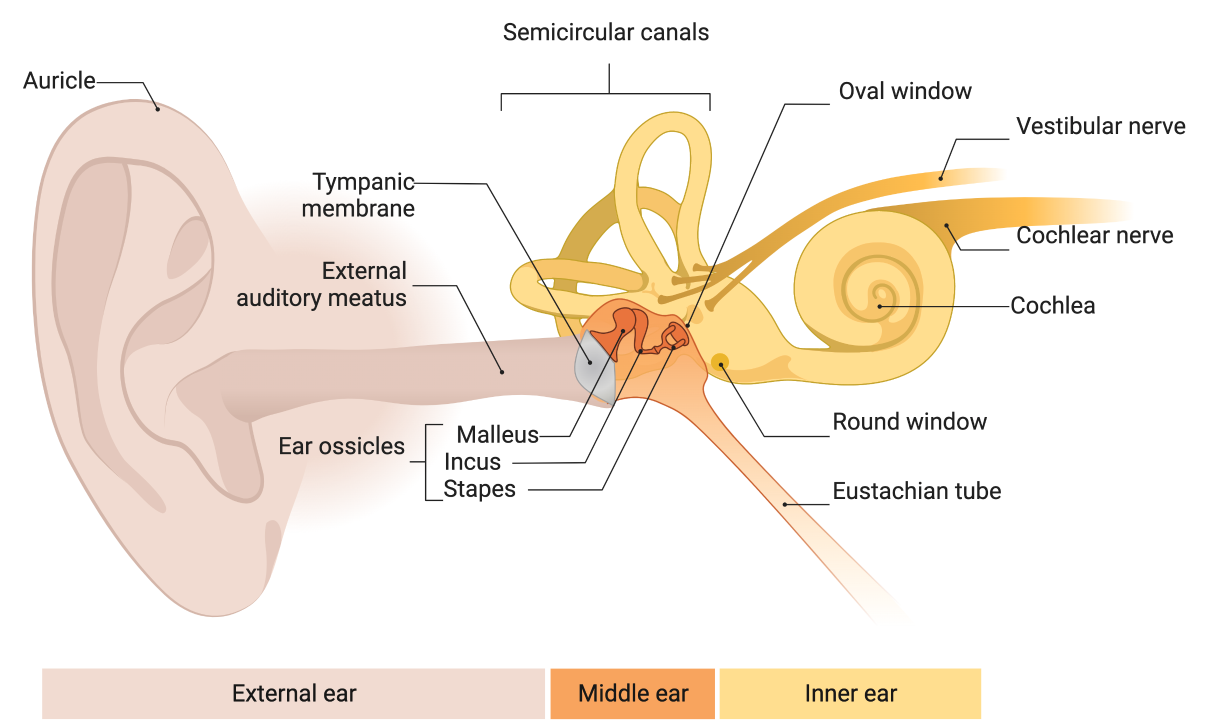
This diagram illustrates different sections of the auditory system.
The prevalence of hyperacusis in the general population is about 15%. More than 30% of people seeking help for their tinnitus and about 80% of people with severe tinnitus report hyperacusis too. It is also known that hyperacusis is more prevalent among children with autistic spectrum disorder than the general population.
In some people, hyperacusis can cause high levels of stress, poorer mental and physical health, and lower quality of life than the general population.
In patients with hyperacusis, it seems that neurons that normally respond at higher sound levels begin to respond to sounds with lower levels, leading to the perception of increased loudness. Hyperacusis leads to experience of negative emotional reaction to certain loud sounds. When a sound induces negative emotions, such as anxiety, fear, annoyance, anger, etc. then the auditory system amplifies that sound leading to the worsening of hyperacusis symptoms. For majority of people who have hyperacusis there is no other underlying health condition.
For majority of people who have hyperacusis there is no other underlying health condition. However, in small percentage of people, hyperacusis can be related to an underlying heath condition including Ménière’s disease, facial paralysis, head trauma, depression, anxiety, post-traumatic stress disorder, obsessive compulsive personality disorder, schizophrenia, Williams syndrome, autistic spectrum disorder, Asperger’s Syndrome, dementia, chronic fatigue syndrome, regional pain syndrome, auditory processing disorders, and some forms of hearing loss.
Childhood adversities can have an influence on children’s development and may affect the way individuals respond to stress later in life. There is a strong relationship between childhood exposure to abuse and household dysfunction and self-reported disability in adulthood. Parental poor mental health is an important form of adverse childhood experiences. Research at Hashir International Institute indicated that children whose parents suffered from a mental illness were at higher risk of developing greater hyperacusis handicap as adults compared with those without a childhood history of parental mental illness. This highlights the importance of mental health for our wellbeing as well as for giving our children psychological strength in dealing with stress later in life.
The “gold standard” for diagnosing hyperacusis is through a clinical interview with a specialist audiologist. The audiologist may also use a wide range of questionnaires to help them to better understand your hyperacusis and distinguish it from other sound intolerance disorders such as misophonia, noise sensitivity and loudness recruitment. In some cases, the audiologist may also ask for a recent hearing test or to sign post you to services that can perform further medical and/or psychological evaluations.
There is no quick fix for hyperacusis. However, there are several methods that have been used for hyperacusis management with various degrees of success. Some clinics reported undertaking ear operations to cutting a tendon in the middle ear to reduce noise-induced pain, covering parts of the cochlea from the inside the middle ear to reduce vibrations in the inner ear, and some doctors even claim that cochlear implantation can help hyperacusis.
Hashir International Institute does not recommend any of these procedures for hyperacusis management as the evidence-base for them is extremely poor, side effects are often permanent, and they lack relevant theoretical basis.
Other treatment options are counselling, education, sound therapy, and cognitive behavioural therapy (CBT). To date, CBT is the most evidence-based intervention for hyperacusis management.
At Hashir International Institute, we offer a premier therapy package for hyperacusis rehabilitation based on CBT. CBT helps to understand and manage the emotional, cognitive, and behavioural processes that are often linked to the experience of hyperacusis. This helps to alleviate anxiety, stress, anger, and depressive symptoms by helping the patient to modify their dysfunctional cognitions, ruminations, and safety-seeking behaviours.
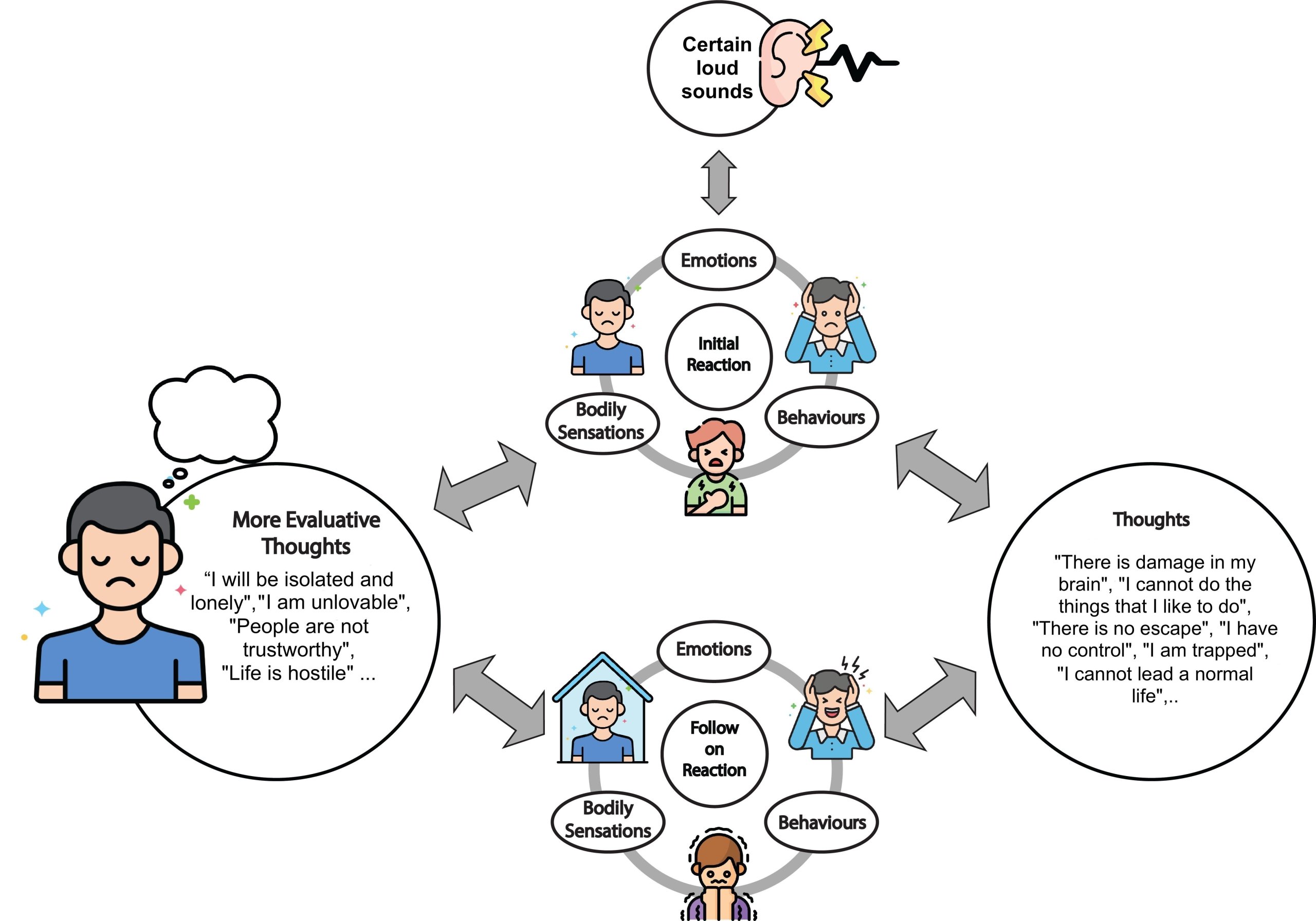
Dr Aazh’s CBT model that explains the experience of distressing hyperacusis.
Over the last decade, Dr Hashir Aazh and his associates have developed several different CBT models for hyperacusis distress. The models have been modified and have evolved based on experiences in clinical practice to be more relevant to the experience of distressing hyperacusis as opposed to general anxiety. Also, the models have been modified so that they can be applicable to most people experiencing distressing hyperacusis. In their most recent model (shown in the diagram above), they conceptualised the distress caused by certain loud sounds in the following way (Figure 3). Perceiving certain sounds creates an initial reaction that includes an emotional component (e.g., feeling upset or irritated), bodily sensations (e.g., tightness in chest, or feeling fullness or pain in the ears), and a behavioural component (e.g., covering your ears). These components are not necessarily triggered by conscious thinking. There are many studies suggesting that the early sensory processing of stimuli is influenced by the emotional significance of those stimuli. This is also the case for certain bodily sensations that often accompany emotions. Certain behaviours can also happen without conscious thinking. Conscious thinking starts after the initial reactions to the triggers and may lead to escalation of the reactions. These thoughts are called automatic thoughts. Some examples of automatic thoughts are “There is damage in my brain”, “I cannot do the things that I like to do”, “There is no escape”, “I have no control”, “I am trapped”, “I cannot lead a normal life”.
The follow-on reactions may also have components related to emotions (e.g., fear or anxiety), behaviour (e.g., using ear protection to avoid noise, self-isolation and avoid going to certain places because of the noises that you may have to face, or reassurance seeking) and bodily sensations (discomfort in ears, headache, tension, or palpitations). The follow-on reactions may lead to further negative thoughts and confirm negative core beliefs. These thoughts will feed back to the reactions, creating the vicious cycle of distress. When the vicious cycle forms, this makes it harder for our brain to recalibrate itself and not to over-amplify certain sounds; instead, it focuses on them even more. The aim of CBT is to break this vicious cycle by teaching the individual skills to help them (1) to identify their thoughts and behaviours, (2) assess if they are helpful or counter-productive, and (3) to change their unhelpful thoughts and modify their avoidance and ritualist behaviours if needed.
CBT is not aimed at directly reducing the perceived loudness of the noises or any discomfort that they may be causing. Rather, the goal is to break the vicious cycle illustrated in the CBT model, which is triggered by the noises. This will allow the brain to re-calibrate itself and not to over-amplify certain sounds over time. Over the last 2 decades, Dr Hashir Aazh and his associates have developed a premier therapy package for hyperacusis rehabilitation based on CBT comprising 14 therapy sessions (via video calls) comprising four stages: I) Assessment, II) Preparation, III) Active treatment, and IV) Maintenance stage. The content of the therapy briefly comprises (1) education about hyperacusis and relevance of CBT, (2) enhancing patient’s motivation to engage with the therapy process, (3) setting goals, (4) formulation, (5) identifying troublesome thoughts, (6) identifying avoidance behaviours and rituals, (7) SEL (Stop Avoidance, Exposure, & Learn from it), (8) KKIS (Know, Keep on, Identify, Substitute), (9) identify and challenge deeper thoughts and beliefs, and (10) integrating CBT into lifestyle (CBStyle). Results from 48 patients who received Hashir International Institute’s premier therapy package of 14 CBT sessions for tinnitus, hyperacusis or misophonia show that CBT delivered via video calls is very effective in reducing the impact of tinnitus, hyperacusis and misophonia.
Aazh, H. (2023). What is Hyperacusis? Available at: https://hashirtinnitusclinic.com/hyperacusis/ (Accessed: Day Month Year)
International Expert Ranking
Dr Aazh is recognised as the number one expert in hyperacusis in Europe during the years 2013-2023 from an independent ranking of biomedical experts (click here to view source).



