Misophonia is defined as decreased tolerance to certain harmless daily sounds, known as ‘triggers’, that seem to be repetitive, and pattern based. Although some scientists believe that misophonia is a ‘disorder’, it is still up for debate. It is possible that the experience of misophonia has a spectrum and on one end it can be a disorder and on the other end it may represent a less common presentation of natural human variation.
The triggers cause unpleasant feelings, emotional distress, physiological and behavioural dysfunctions ranging from mild to severe. Once the trigger is detected by the individual experiencing misophonia, they get hyper-focused on them and cannot distract themselves. The severity of emotional reactions to these triggers may substantially be different from one person to another. Misophonia can impair the individual’s occupational, academic, and social activities and cause interpersonal problems. The onset of misophonia is often in late childhood and early adolescence (e.g., 10 to 12 years old). Misophonia can happen with or without misokinesia which is defined by oversensitivity to seeing people eating, drinking, jiggling legs etc.
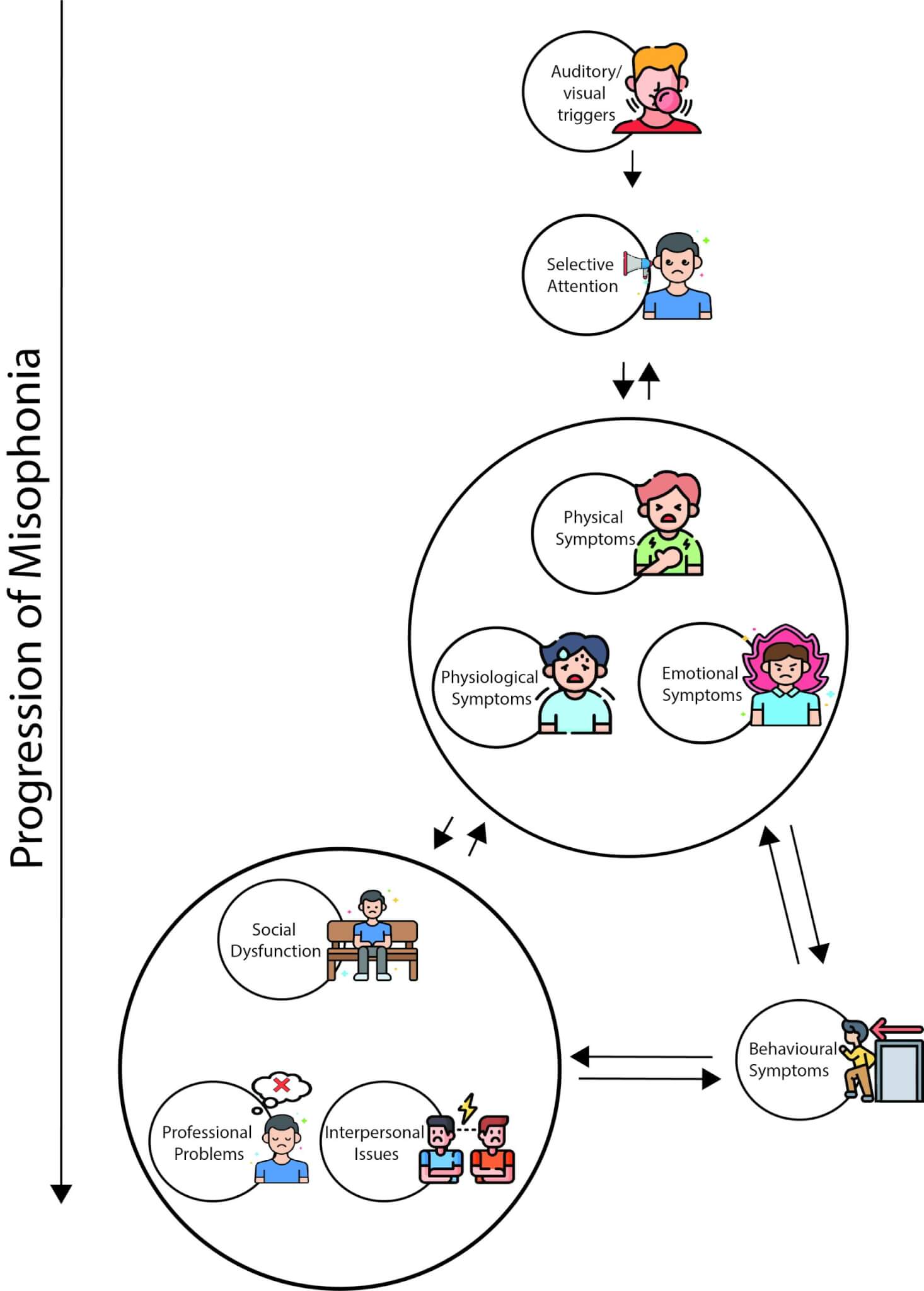
This diagram demonstrates the progress and the vicious cycle of misophonia, starting with exposure to trigger, followed by selective attention on those triggers which leads to bodily sensations and emotional distress. These experiences may result in avoidance and/or ritualistic behaviours which in turn limit various aspects of the individual’s life. For example, it can impact on their work/school, relationships with friends and family, and cause interpersonal problems. The more the person’s life is influenced by their misophonia, the more important it becomes and the selective attention on triggers will rise leading to increased severity of misophonia.
It seems that misophonic reactions are not related to the loudness of the triggers. The triggers can be grouped as (1) mouth and nasal sounds, (2) human-related but not mouth and nasal sounds, and (3) environmental sounds. There is a wide range of auditory triggers reported by individuals experiencing misophonia, however, mouth and nasal triggers seem to set off most individuals with misophonia. Misokinesia triggers (i.e., visual triggers) can be associated with the misophonia triggers (e.g., hearing and seeing someone biting an apple) or not associated with them (e.g., seeing someone fidgeting with their hair). Regardless, the most common misokinesia triggers are jiggling, swinging legs, fast blinking, and constant eye movement.
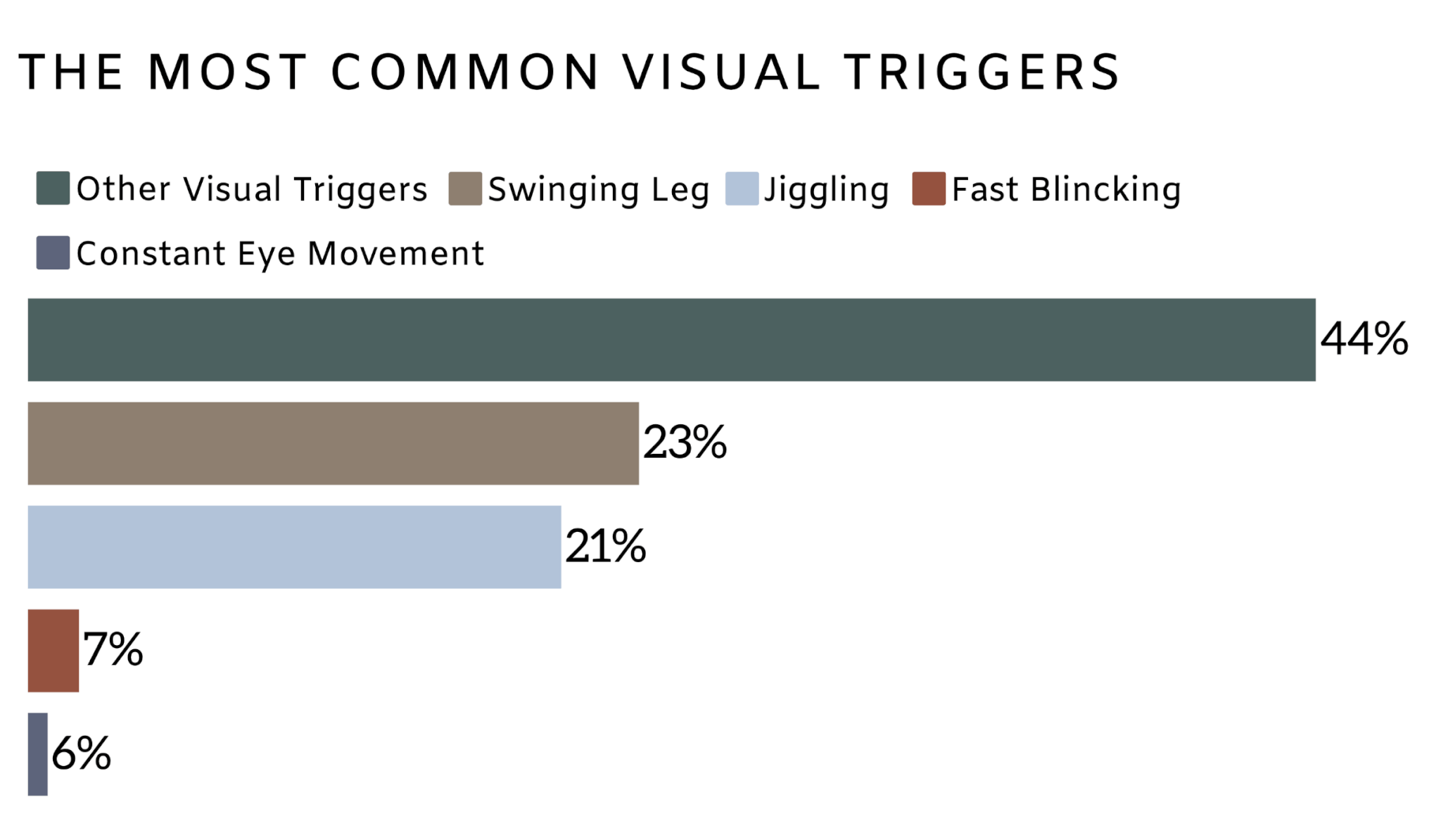
This bar diagram shows the distribution of visual triggers based on a study on 301 individuals with different severity of misophonia. The numbers represent the percentage of each trigger across study participants.
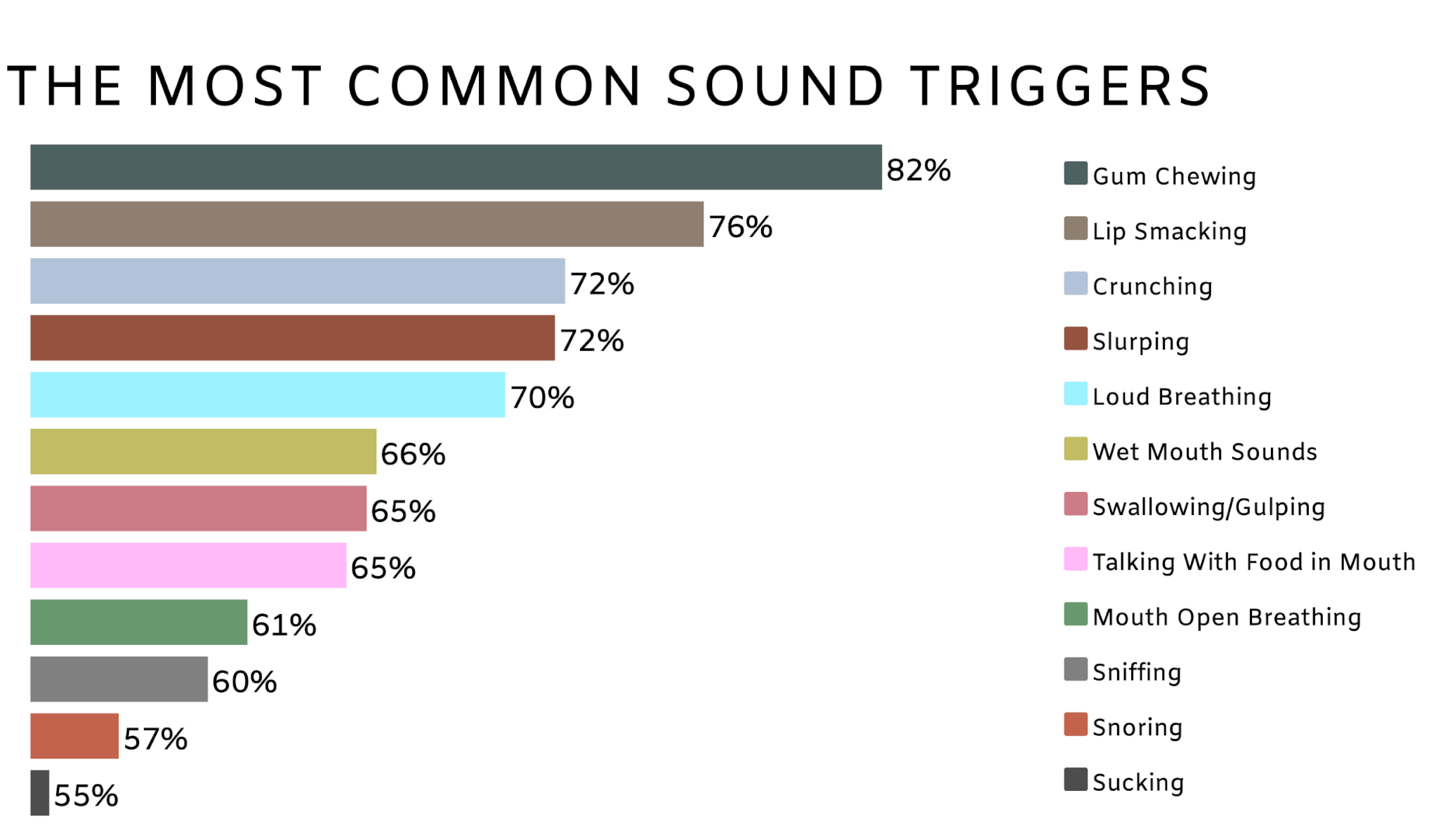
This diagram shows twelve most common sound triggers among 301 self-reported individuals with different severity of misophonia. The values show the percentage of each trigger in study participants.
When the person with misophonia hears (or sees) the triggers (e.g., chewing), they may experience pressure in chest, arms, head or whole body and clenched jaw or teeth or tightening of their muscles. In addition, they may sweat, or feel increased heart rate and temperature or blood pressure. These bodily experiences are similar to when we are very angry, anxious, disgusted or scared.
Physiological symptoms are the symptoms that occur when you feel anxious, scared, or angry such as increased heart rate, blood pressure, and sweating. Physical symptoms refer to all the physical sensations such as headaches, back pain, muscle aches, joint pain, chest pain, shortness of breath and suffocation (Figure 5).
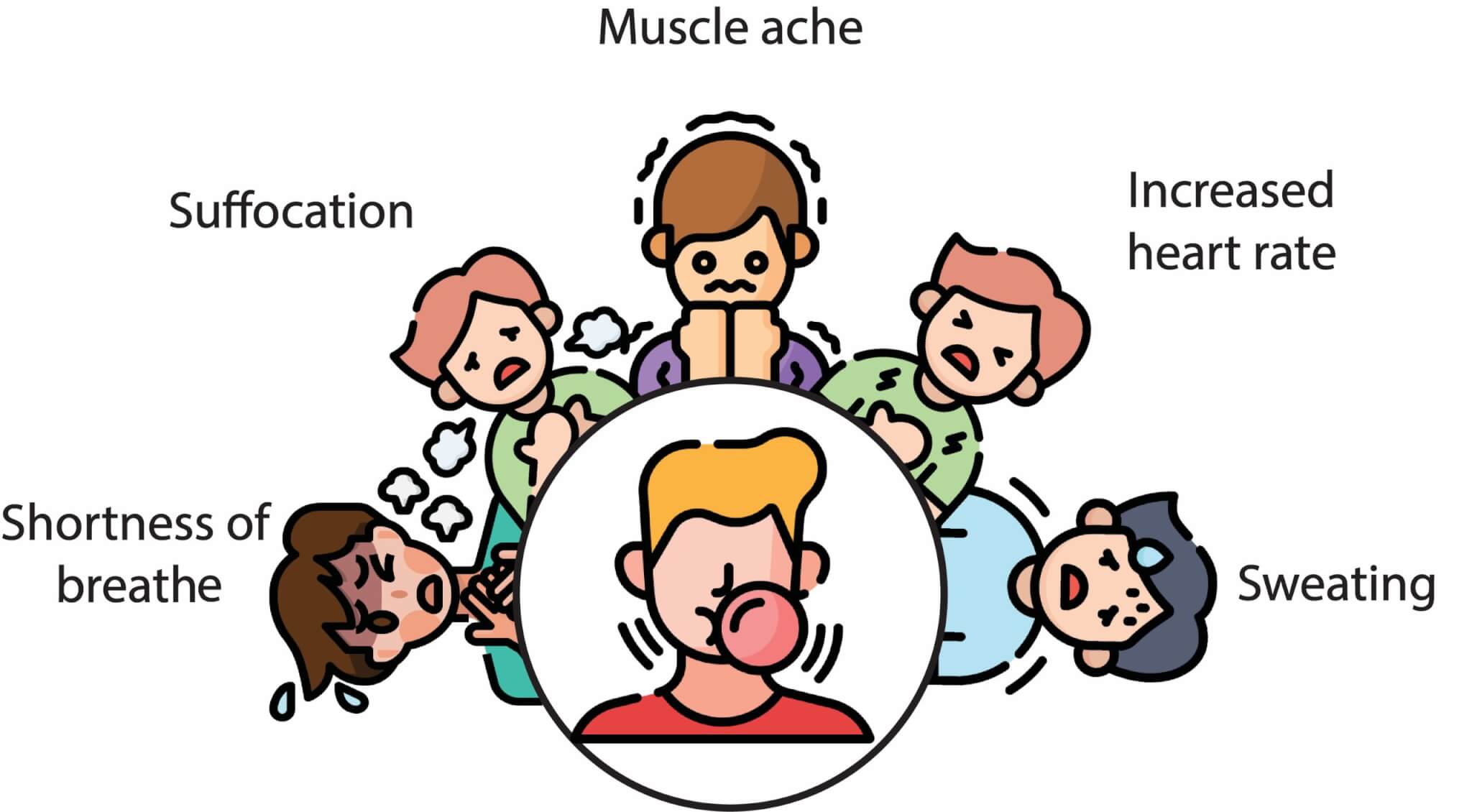
This figure shows different physiological and physical responses.
Following the exposure to misophonic triggers, individuals may experience anger, irritation, disgust, anxiety, or even rage toward the source of the sounds which can be another person. The reaction is typically stronger if triggers are made by a family member. Most individuals with misophonia do not seem to react as strongly if the trigger is generated by a stranger or self-generated.
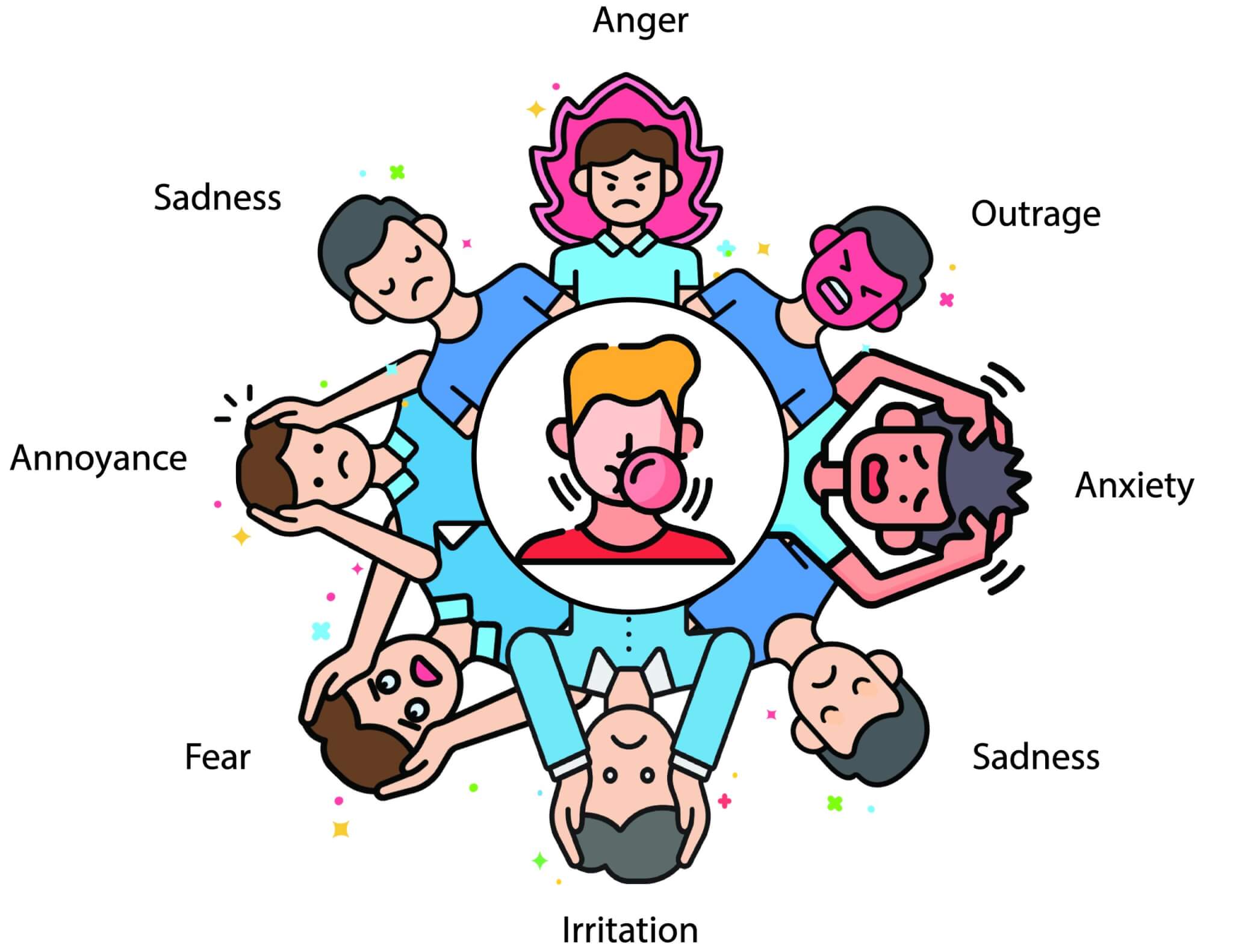
This figure shows different emotional responses.
Due to the distress misophonic triggers cause, the individual develops certain behavioural reactions like agitation and aggression mostly toward the sound source which may in a few cases turn to physical aggression. The behavioural reactions may differ across children and adults with misophonia, while children may show verbal and physical outbursts and tantrums, it is more under control in adults which does not necessarily negate the distress they endure. Sufferers learn to take strategies to reduce the agony and symptoms: avoiding appearance in the situation with the risk of triggers (e.g., dinner time with the family), escaping the situations with the triggers (e.g., leaving the dinner table), or ritualistic behaviours such as mimicking the triggers. The behaviours of the individuals experiencing misophonia may also impact on the psychological health and wellbeing of the people close to them (e.g., partners, family members, etc).
The level of impairments depends on the severity of misophonia. However, how much it impacts on the person’s life depends on a variety of factors ranging from the severity of misophonia and the functional impairments it creates to the person’s mental and general health status, and family and social support network available to them. For some people, misophonia can interfere with day-to-day life influencing their general psychological well-being. Due to the hyper-focus on the triggers, the individual may experience concentration difficulties, leading to dysfunction in professional/work-related tasks and academic performance especially in circumstances where authorities (employers/teachers) lack understanding about misophonia and do not accommodate the sufferer’s needs. To avoid the triggers if it is associated with a certain individual (e.g., a close friend), the social network and interpersonal aspects of the person’s life can be affected leading to social isolation and increasing risk of developing psychological disorders.
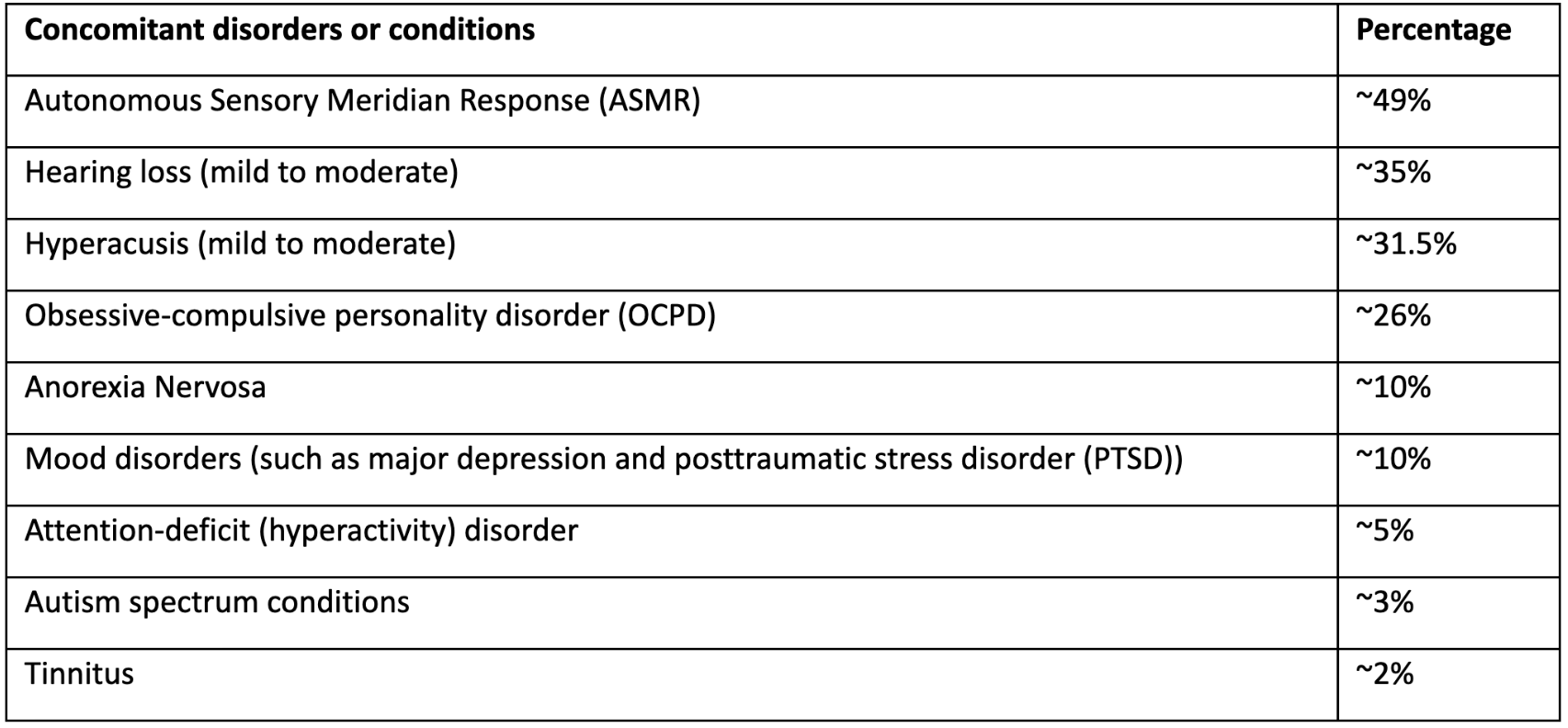
Misophonia can be present in individuals with or without auditory conditions, psychiatric disorders, and neurodevelopmental/neurological symptoms. Having said that, it is not fully understood if these disorders increase the risk of misophonia or misophonia leads to the development of these disorders. It is important to mention that the prevalence of comorbid disorders reported in various research studies depend on the study population. For example, if the patients are selected from a psychiatric clinic, then the incidence and level of psychiatric disorders are higher while if they are selected from an audiology clinic, then the number of concurrent audiological conditions are higher. The prevalence of concurrent disorders is lower in studies in which patients were selected from the general population. This may suggest individuals who have misophonia combined with other conditions are more likely to seek professional help compared to those with standalone misophonia. The table below lists results from a mix of clinical and non-clinical populations.
Percentage of audiological, psychological, and medical conditions among patients who experience misophonia. This table is generated based on several research studies in different populations and countries.
In summary, misophonia is a complex condition, characterised by decreased tolerance to certain sounds or even visual stimuli (in the case of misophonia combined with misokinesia), followed by several physical, physiological, emotional, and behavioural symptoms that can cause mild to severe disabilities in different aspects of the sufferers’ lives. Misophonia may and may not co-occur with psychiatric, neurological, and audiological conditions.
There are several explanations why individuals who experience misophonia perceive the trigger sounds negatively, although others may not even pay attention to them. Studies show that in people with misophonia some parts of the brain seem to work differently hence giving rise to the negative experiences. One example is a section deep in the middle of the brain, called insula. Insula is responsible for emotions such as disgust, interoception, emotional processing, emotional regulation and processing of saliency.
The human brain contains billions of nerve cells (aka neurons) arranged in patterns that coordinate tthoughts, emotions, behaviours, movement, and sensation. A complicated highway system of nerves connects the brain to the rest of your body, so communication can occur in split seconds. An adult human brain has almost ~85 billion neurons that some of them are connected to each other which makes almost 100 trillion neuronal connections. For controlling our actions (e.g., decision making or movement), several parts of the brain work together as a network not just a spot of the brain, so it is important that these brain parts are well-connected and send each other signals to work together in harmony. Scientists can detect the activity of different brain parts by using several methods like fMRI (Functional magnetic resonance imaging). fMRI shows which parts of the brain are activated via comparing oxygen use among them (more oxygen use indicates more brain activity). Sometimes due to psychiatric or neurological disorders, different parts of the brain do not work normally (e.g., either overactive or under-active). Or sometimes different parts of the brain are connected with one another although they should not, so it leads to abnormal responses.
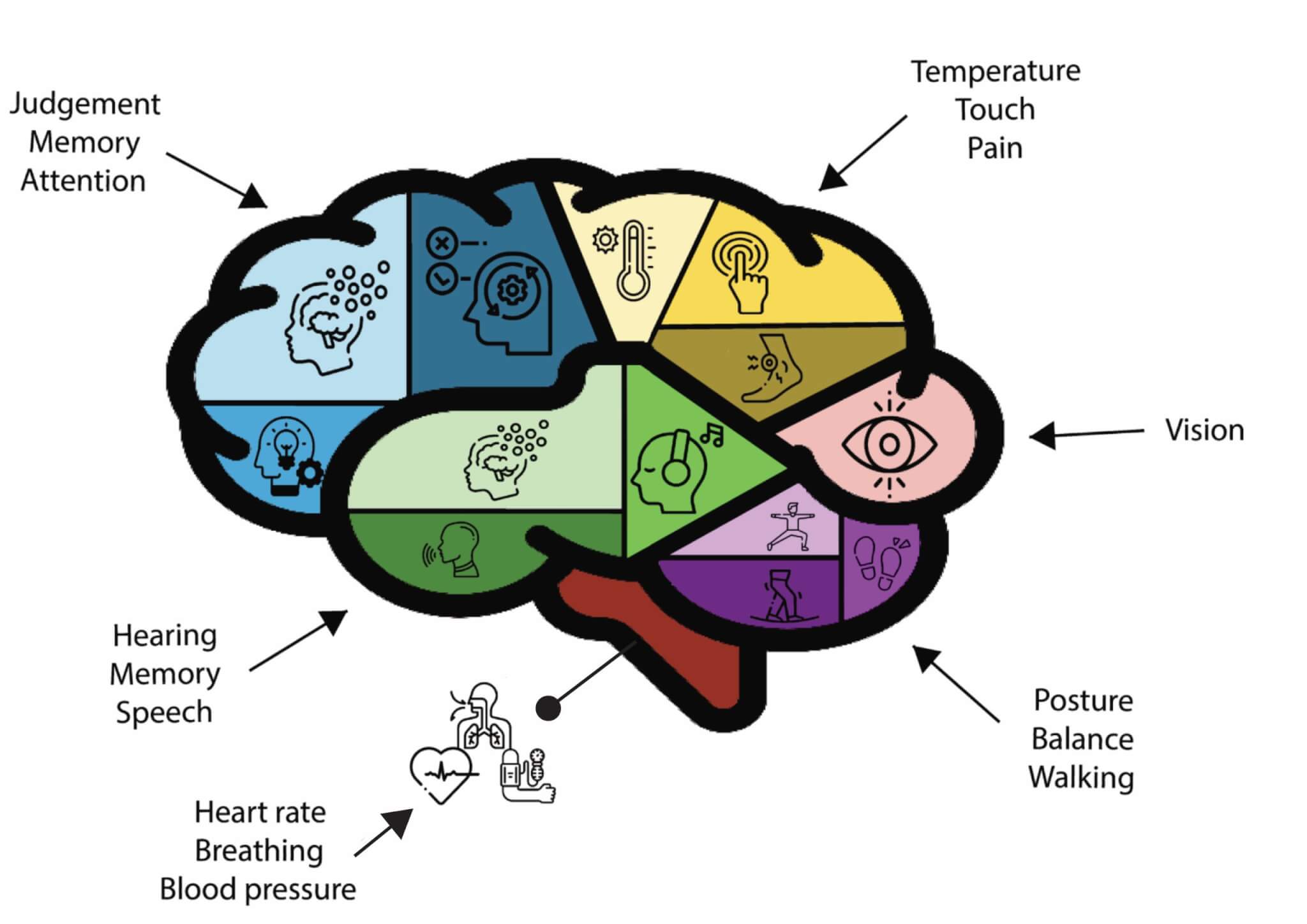
This image shows the whole brain with four lobes, cerebellum, and brainstem. Some of the most common responsibilities of the frontal lobe (blue) are attention, memory, and judgement. Parietal lobe (yellow) three main functions are touch sensation, regulating body temperature and pain. Occipital lobe (pink), the smallest brain lobe is responsible for vision and interpretation of visual information. Temporal lobe (green) is known to control memory, hearing, and speech. The Cerebellum (purple) is responsible for walking, balance, and posture. Brainstem (red) regulates breathing, heart rate and blood pressure. All these brain regions have more functions than mentioned here.
Each brain hemisphere (parts of the cerebrum) has four sections, called lobes; frontal lobe with lots of sub-regions that are responsible for all cognitive functioning like memory, decision making, attention, etc and it is located in the front part of our skull, it is considered as the biggest lobe which completes around age of 25. Then comes the parietal lobe, roughly located at the upper back area in the skull with numerous sub-regions like the motor cortex. It processes sensory information it receives from the outside world, mainly relating to touch, taste, temperature, etc. At the back of the head, the occipital cortex is situated, which is responsible for visual perception, including colour, form, and motion. The temporal lobe on both sides of our ears primarily is responsible for interpreting sounds from the ears and plays a significant role in recognizing and using language. Besides, there are several subcortical regions (below these lobes) that control emotions like the limbic system with amygdala and hippocampus lying in it. Underneath the limbic system, brainstem and cerebellum are located, regulating balance, breathing, heart rate and walking, posture, and coordination (Figure 7). It is important to highlight that each part of the brain has many more functions that have not been mentioned here.
Motor cortex, almost on the top of our skull stretched down to the top of both ears, directs the movement of the body. As demonstrated in Figure 8, each part of the motor cortex is responsible for the movement of body parts starting from legs, feet, hip, and trunk on the top, followed by hands, arms, fingers, face, tongue, and larynx (Figure 8).
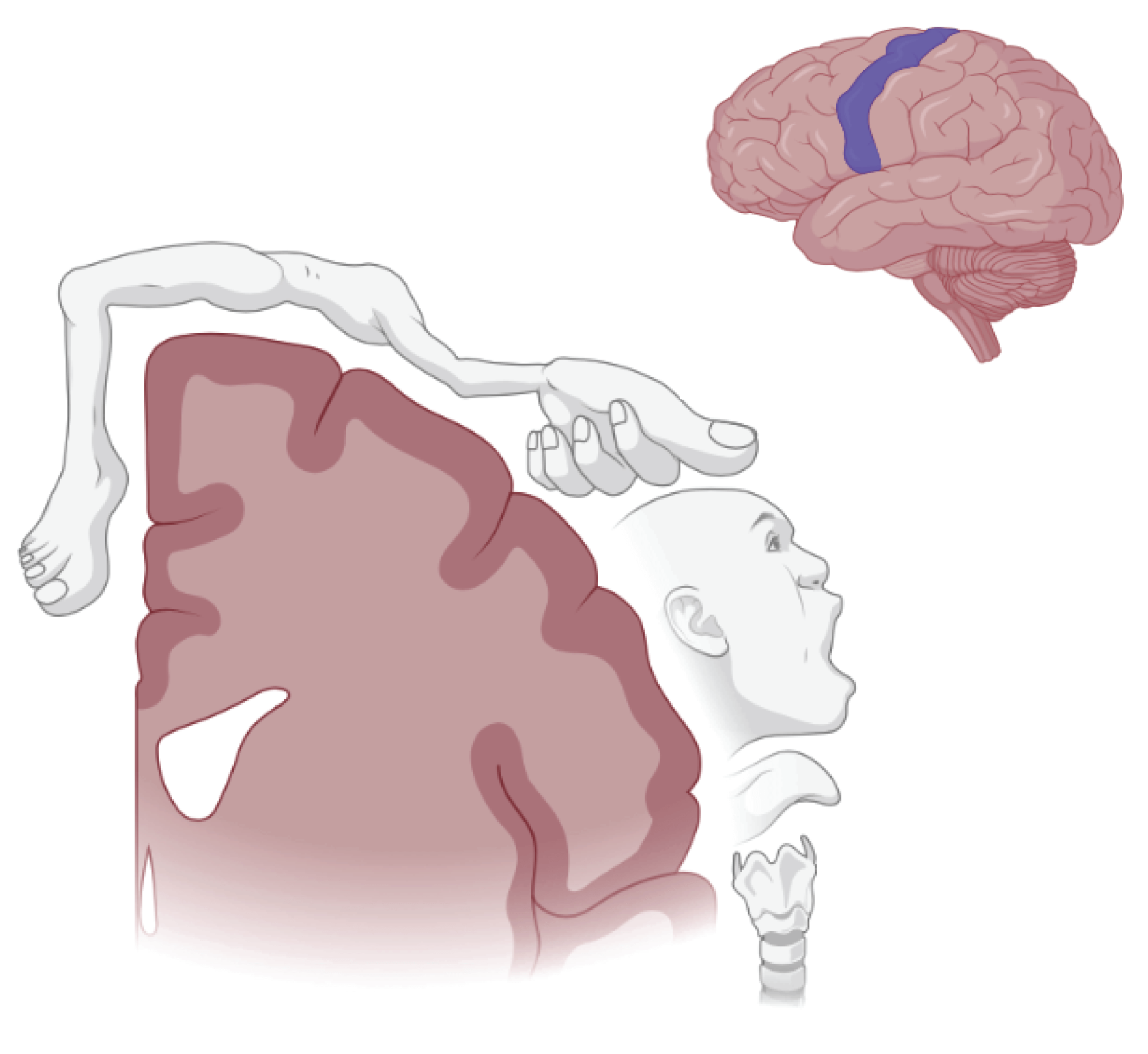
This figure shows the motor cortex in the brain and from the front view with allocated parts controlling the movement of different body parts.
Interoception is a lesser-known sense that helps us to understand and feel what's going on inside our body. For example, it helps us to realise if we are hungry, hot, or cold. Research shows that individuals with misophonia feel or perceive their bodies differently which seems to be controlled by a part of the brain known as insula cortex which sits deep in the middle of the brain.
This figure represents interoception, a lesser-known sense that helps us understand and feel what's going on inside our body and our visceral sensations (inside body organs) such as feeling our heart beating or stomach cramp.
Imagine you are driving on a busy and noisy road; you are aware that the street is noisy but none of the sounds stand out. While you are driving, an ambulance approaches and grasps your attention to go out of its way so it can drive to the nearest hospital. In this scenario, the sound of an ambulance siren is salient. Although the road was noisy, it still drew your attention. Directing your attention to the sound of ambulance sirens among all other environmental sounds is assumed to be regulated by the insula.
The figure above shows an example of a salient sound; ambulance sound standing out among other sounds in the acoustic environment.
Emotional regulation is adjustment of our emotions in response to situations. People with anger issues have problems with emotional regulation. In misophonia, the region responsible for emotional regulation is overactive and overconnected to the other parts of the brain like the amygdala, hippocampus.
Amygdala consists of two tiny almond-shaped structures in the middle and both sides of the brain, responsible for memory, decision-making and emotional responses like fear, anxiety, and anger.
Hippocampus is the main region for memory encoding, storing and processing. In other words, the hippocampus helps our short-term memory to transfer to long-term memory (known as memory consolidation). The damage in the hippocampus results in forgetfulness or amnesia. Both parts are subregions of the limbic system. In misophonia instead of damage to the limbic system, it seems that there is over-connection between these regions leading to overcommunication among them. For instance, imagine you enter your house at night and click the light switch in your hallway but instead of the hallway lights, all lights in your house plus the alarm system, kitchen appliances, TV and vacuum cleaner turn on. ‘Switching the light on’ is like hearing the triggers, and all lights and other appliances turning on is like lightening up the brain parts that should not be lit up or activated. So, when insula detects misophonia triggers among all other sounds in the environment, it does activate several parts of the brain that should not be activated. Like the insula, the cingulate cortex, regulating saliency, is also involved in abnormalities observed in misophonia.
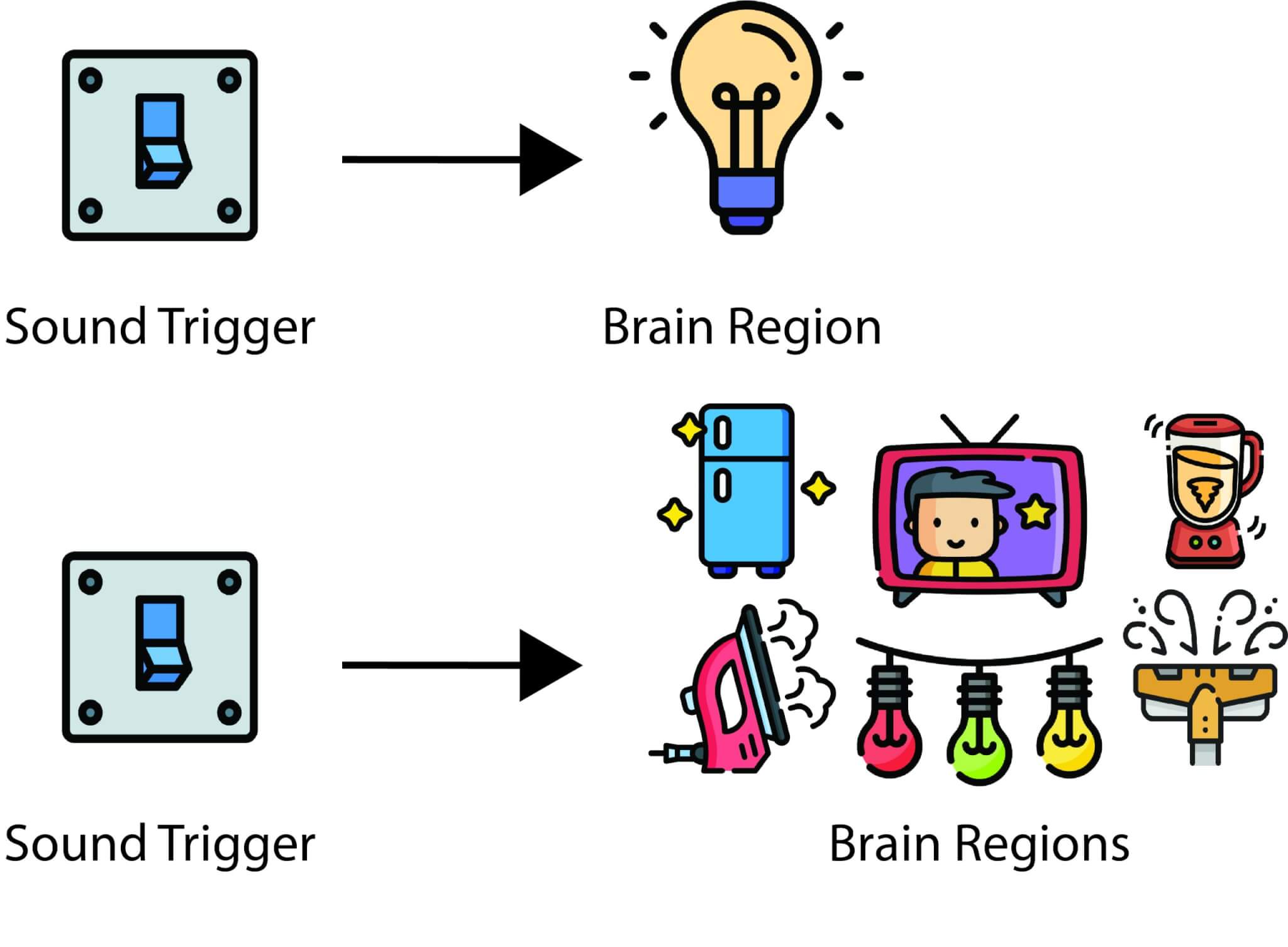
This figure shows the differences in brain functions of non-misophonics (top) and misophonic sufferers (bottom). The light switch represents the sound trigger which leads to activation of a certain region or network in the brain (e.g., auditory cortex) in non-misophonics. However, in misophonics the sound trigger (light switch) causes the activity of several unrelated brain regions (e.g., appliances).
It is possible that the insula in brains of people with misophonia pays more attention to the trigger sounds (e.g., gum chewing) and since insula is over-connected to amygdala, hearing those sounds leads to negative emotions (e.g., anger). Insula can also be over connected to a part of the frontal cortex and cingulate cortex or medial cortex which explains why some people who experience misophonia are unable to disengage from paying attention to the trigger sounds (Figure 12). This is important to know since individuals with misophonia report to become ‘hyper-focused’ or ‘hooked’ to the triggers once they encounter them, and it is difficult to distract from the trigger. This can become more complicated as the frontal cortex is also responsible for self-control, decision-making and morality (principles concerning the distinction between right and wrong or good and bad behaviour).
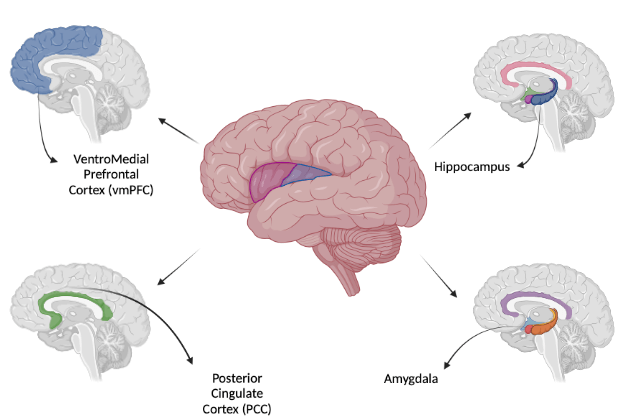
This image shows the connection between insula and other parts of the brain that play a role in the experience of misophonia. The insula is colour coded in blue and purple in the middle of the brain.
Another reason why sufferers experience misophonia is because a small part of the motor cortex, almost on top of our skulls laterally down to our ears that controls our movement and sensations, is also overconnected with hearing and vision parts of the brain as well as with insula. This over connection explains the progression of misophonia. Individuals with misophonia experience negative emotions (regulated by the insula and amygdala), once they hear (through hearing parts of the brain) or seeing others chewing (through seeing part of the brain) in response to mouth and nasal sounds or body movement sounds that are controlled by motor cortex. This suggests that the over-connection between the seeing and hearing and motor/movement cortex unwantedly and involuntarily activates the “mirror system” in the motor cortex of the sufferers (Figure 13).
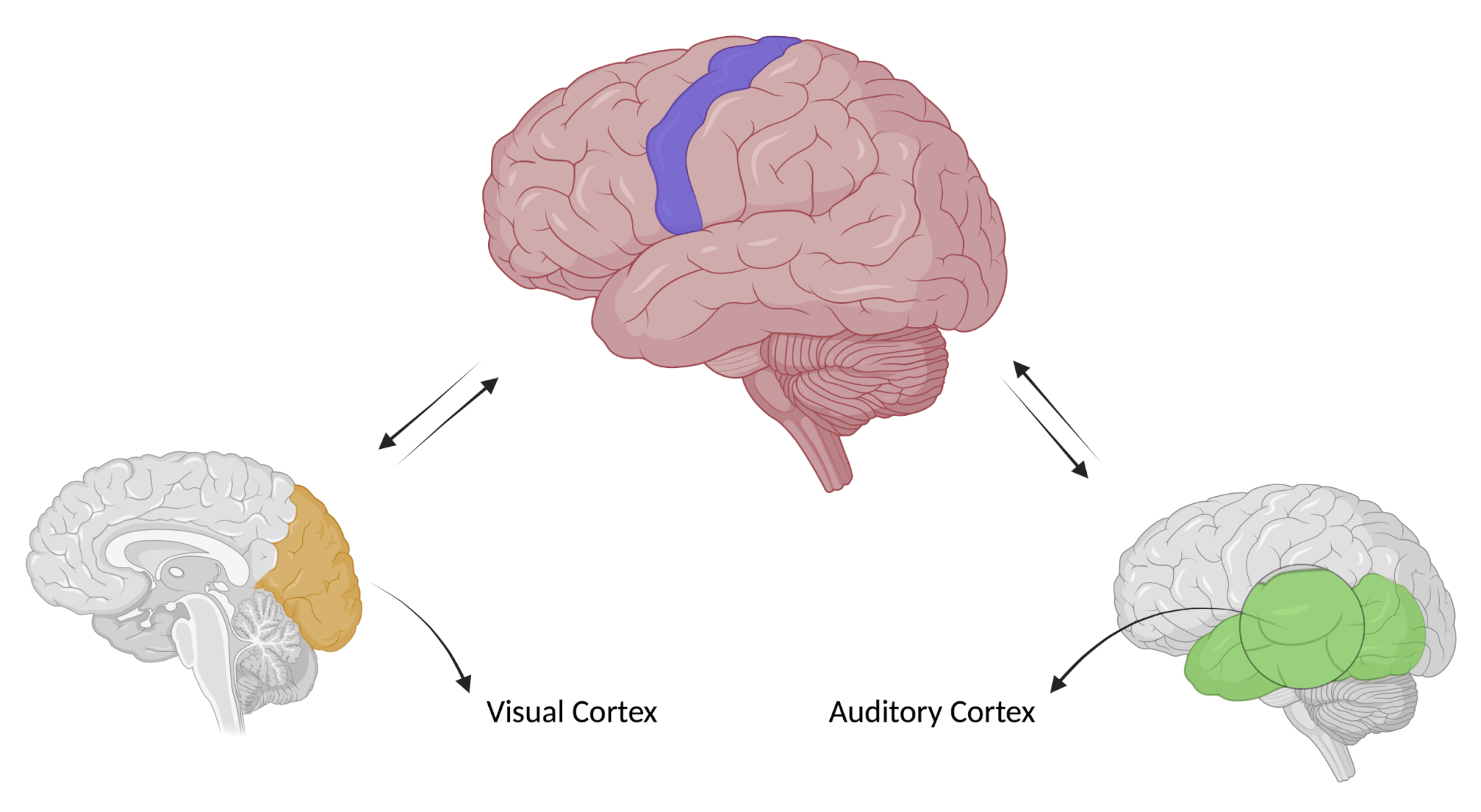
This image illustrates the connection between motor-cortex, auditory and visual parts of the brain.
The (pre)motor cortex is the densest part of the brain with mirror neurons. Mirror neurons are known to be involved in learning and social behaviour. Mirror neurons are the reason we may yawn when we see others yawn or smile if we see another person smile. Mirror neurons are also thought to underlie empathy like when we see someone in pain, we feel empathy and become sad for the person suffering. Mirror neurons are a type of motor neurons that fire/activate when we act or see actions performed by another individual (Figure 14). Mirror neurons in pre-motor cortex seem to get activated (known as hyper-mirroring) when the individual with misophonia sees or hears other people produce the triggers which may result in negative experiences. These triggers results in negative experiences in misophonia sufferers, given that they are highly distracting and seem to take control of sufferers.
This figure represents a mirror neuron that lights up when we observe another person doing an action.
To sum up, once a sufferer is exposed to a trigger several parts of their brain lighten up. These regions are responsible for emotional processing, saliency, disgust, anger, seeing and hearing.
There are several treatments proposed for misophonia including cognitive behavioural therapy (CBT), education and sound therapy (known as retraining therapy), exposure therapy, eye movement and desensitisation reprocessing (EMDR), psychopharmacological therapy (such as beta-blockers, antipsychotic, and selective serotonin reuptake inhibitor (SSRI) drugs), counterconditioning therapy (a form of behavioural treatment), and acceptance and commitment therapy (ACT). Among all these treatments, only the short and long-term (3, 6, and 18 months) effects of CBT has been investigated in a randomised clinical trial (RCT) and the effectiveness of other treatments is still debatable. To evaluate the effectiveness of a particular treatment, it is necessary to compare the results for a group of people receiving the treatment with the results for a matched “control” group. The control group may receive no treatment (for example they may be put on a waiting list), in which case they are referred to as a “passive” control group. Alternatively, the control group may receive some other form of treatment or therapy, in which case they are called an “active” control group.
At Hashir International Specialist Clinics, we offer a specialised misophonia rehabilitation programme based on CBT. CBT helps to understand and manage the emotional, cognitive, and behavioural processes that are often linked to the experience of misophonia. This helps to alleviate anxiety, stress, anger, and depressive symptoms by helping the patient to modify their dysfunctional cognitions, ruminations, and safety-seeking behaviours.
Over the last decade, Dr Hashir Aazh and his associates from the Royal Surrey hospital and University of Cambridge have developed several different CBT models for misophonia distress. The models have been modified and have evolved based on experiences in clinical practice so as to be more relevant to the experience of distressing misophonia as opposed to general anxiety. Also, the models have been modified so that they can be applicable to the majority of people experiencing distressing misophonia. In their most recent model (Figure 15), they conceptualised the distress caused by misophonia in the following way. Exposure to the triggers create an initial reaction that includes an emotional component (e.g., feeling annoyed or irritated), bodily sensations (e.g., increased heart rate, tingling sensation behind ears), and a behavioural component (e.g., looking at the sound source, mimicry, shouting). These components are not necessarily triggered by conscious thinking. There are many studies suggesting that the early sensory processing of stimuli is influenced by the emotional significance of those stimuli. This is also the case for certain bodily sensations that often accompany emotions. Certain behaviours can also happen without conscious thinking. Conscious thinking starts after the initial reactions to the triggers and may lead to escalation of the reactions.
The follow-on reactions may also have components related to emotions (e.g., fear or disappointment), behaviour (e.g., avoiding certain people or activities, asking people to not to make noise, or reassurance seeking) and bodily sensations (tension or palpitations). The follow-on reactions may lead to further negative thoughts and confirm negative beliefs. These thoughts will feed back to the reactions, creating the vicious cycle of distress. When the vicious cycle forms, this makes it harder for our brain to put the trigger sound into the background; instead, we focus on it even more. The aim of CBT is to break this vicious cycle by teaching the individual skills to help them (1) to identifying their thoughts and behaviours, (2) assessing if they are helpful or counter-productive, and (3) to change their unhelpful thoughts and modify their avoidance behaviours if needed.
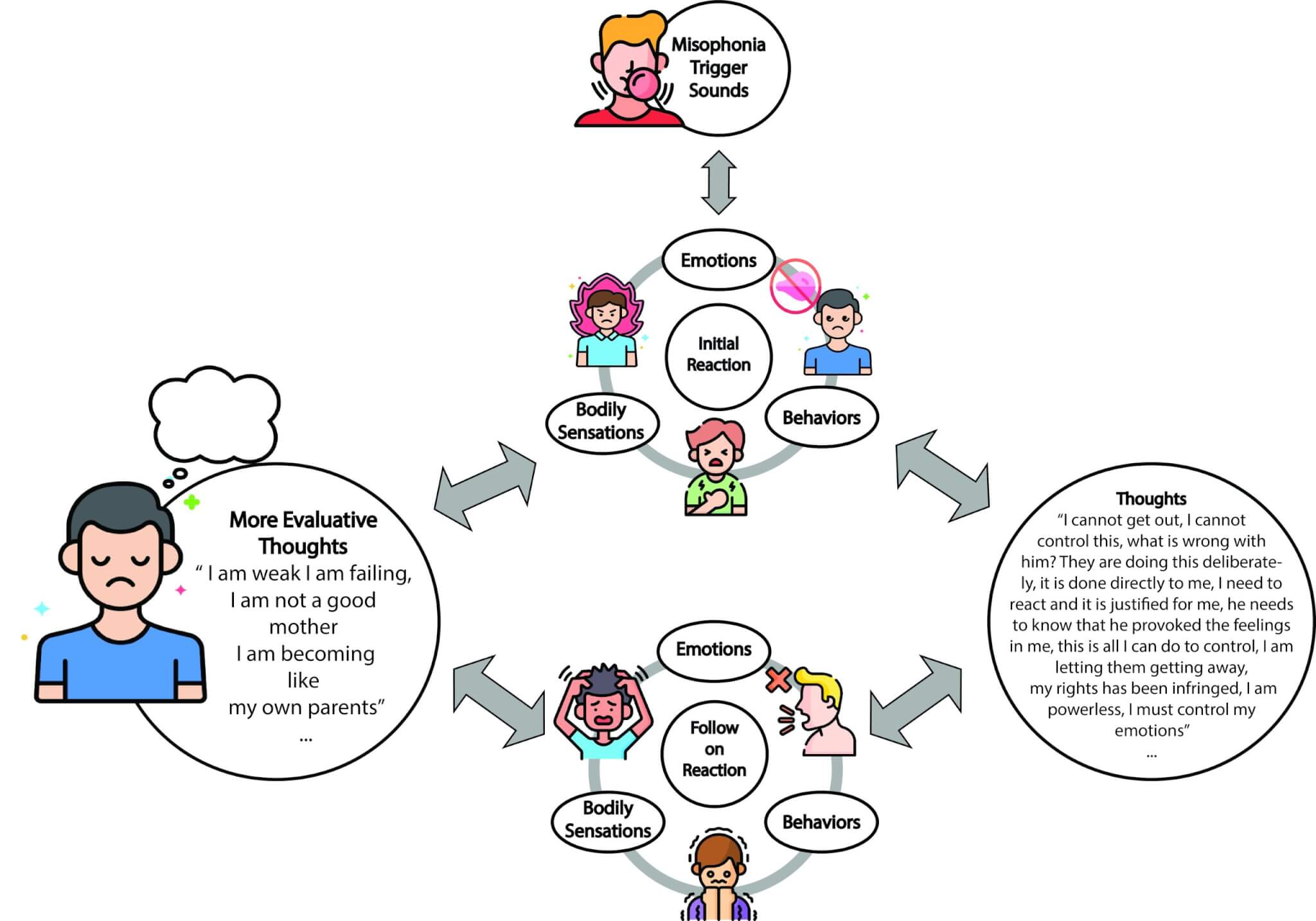
Dr Aazh’s CBT model that explains the experience of distressing misophonia.
At the 6th International Conference on Hyperacusis and Misophonia (1-2 July 2022, Birkbeck College, University of London), Dr Hashir Aazh presented results of a programme of audiologist-delivered CBT comprising 14 therapy sessions (via video calls). This is a specialised therapy for misophonia rehabilitation and comprises four stages: I) Assessment, II) Preparation, III) Active treatment, and IV) Maintenance stage. The content of the therapy briefly comprises (1) education about misophonia and relevance of CBT, (2) enhancing patient’s motivation to engage with the therapy process, (3) setting goals, (4) formulation, (5) identifying troublesome thoughts, (6) identifying avoidance behaviours and rituals, (7) SEL (Stop Avoidance, Exposure, & Learn from it), (8) KKIS (Know, Keep on, Identify, Substitute), (9) identify and challenge deeper thoughts and beliefs, and (10) integrating CBT into lifestyle (CBStyle). The data for 42 patients enrolled and completed the therapy programme were reviewed. Out of 42 patients, 24% had tinnitus alone, 5% had hyperacusis alone, 38% had misophonia alone, 26% had tinnitus combined with hyperacusis, 2% had hyperacusis combined with misophonia and 5% had all three conditions. 22% of the patients were children, mean age was 12 years old (ranged between 8 to 15 years). The mean age for adults was 43.8 years (ranged between 17 and 69 years old). Prior to the start of the therapy, 65% of patients had at least one psychological symptom that needed to be referred to mental health services. This reduced to 37% after the therapy. The mean score on Misophonia Impact Questionnaire (MIQ) reduced from 16 (out of maximum score of 24), before treatment to 8.3 (out of maximum score of 24) after treatment. Patients’ confidence in managing their symptoms as measured via the 4C questionnaires (0 means not confident at all and 100 means fully confident in managing their symptoms) improved from 10% before treatment to 40% confident in managing their misophonia after the treatment. This study was not a controlled trial. There is only one controlled trial on CBT for misophonia which has been conducted by a team of psychiatrists in Amsterdam. Their study showed that CBT delivered in a group setting helped sufferers reduce their misophonia symptoms by about 30%.
At Hashir International Specialist Clinics, we do not offer this treatment.
Retraining therapy also known as tinnitus retraining therapy (TRT) is another method for misophonia treatment. It is a form of habituation therapy, originally designed for the treatment of tinnitus. TRT has two components. Educational counselling and sound therapy. Educational counselling is supposed to be a crucial part of TRT; it teaches patients the components of the Jastreboff’ s neurophysiological model and encourages them to reclassify their trigger sounds as a neutral signal. Sound therapy is claimed to facilitate habituation by decreasing the strength of the trigger sounds using background noise or music. The TRT protocol requires that the patient adheres to the regimen for 12-24 months, and specifically points out that habituation is a long-term process. To our knowledge there is no clinical trial that assesses the effect of TRT on misophonia.
At Hashir International Specialist Clinics, we do not offer this treatment.
Exposure therapy is administered by listening to the misophonic triggers so many times that they eventually habituate or get used to them. The trigger's playback is repeated enough so the sufferer does not react to them anymore. The effectiveness of this treatment is ambiguous and to our knowledge there is no clinical trial reporting its effect.
At Hashir International Specialist Clinics, we do not offer this treatment.
EMDR involves moving eyes a specific way while distressing and traumatic memories regarding the triggers are processed. EMDR’s goal is to help healing from the emotional distress trauma and negative experiences caused by the triggers. When sufferers undergo EMDR, they access memories and emotional distress caused by the triggers in very specific ways. Combined with eye movements and guided instructions, accessing those memories and distress helps them reprocess what they remember from the triggers. According to a non-controlled study on 10 people, 3 sufferers showed clinically significant improvement. However, there is no controlled clinical trial assessing effectiveness of EMDR on misophonia.
At Hashir International Specialist Clinics, we do not offer this treatment.
Although there are no medications approved for the treatment of misophonia, some medicines have been reported to be effective in reducing the symptoms. Medications like fluoxetine and escitalopram that treat anxiety and depression caused by misophonia symptoms, while beta-blockers reduce the physiological response (e.g., increase heart rate). According to a few case studies, beta-blockers (e.g., propranolol) completely eliminated multiple auditory and visual trigger symptoms related to other people eating. None of the above-mentioned medications have gone through controlled clinical trials.
At Hashir International Specialist Clinics, we do not offer this treatment.
In counterconditioning therapy, the patient needs to listen to the trigger sounds and learn to reduce or eliminate their reaction using various techniques such as meditation, positive imagery for relaxation. However, there is no controlled clinical trial assessing effectiveness of counterconditioning on misophonia.
At Hashir International Specialist Clinics, we do not offer this treatment.
ACT is focused on acceptance, mindfulness, opposite action, and non-judgmental attitude. In this treatment the patient learns to practise describing the triggering situation (such as a person eating) to oneself in a factual, non-judgmental way. ACT commonly uses six core principles to help patients develop psychological flexibility. A) Cognitive diffusion: Learning methods to reduce the tendency to express thoughts, images, emotions, and memories. B) Acceptance: Allowing unwanted private experiences (thoughts, feelings, and urges) to come and go without struggling with them. C) Contact with the present moment: Awareness of the here and now, experienced with openness, interest, and receptiveness (e.g., mindfulness). D) The observing self: Accessing a transcendent sense of self, a continuity of consciousness which is unchanging. E) Values: Discovering what is most important to oneself and focus on them as opposed to being distracted by less important problems. However, there is no controlled clinical trial assessing effectiveness of ACT on misophonia.
Erfanian, M. & Aazh, H. (2023). What is Misophonia? Available at: https://hashirtinnitusclinic.com/misophonia/ (Accessed: Day Month Year).


