Now I Am Confident That I Can Relax, Concentrate on My Work, Sleep Well, and Enjoy My Life Fully Despite Hearing a Loud Tinnitus: A 51 Year’s Old Man With Left-Sided Tinnitus Caused by Working With Loud Machinery Without Ear Protection.

We use a pseudo name David here. David developed tinnitus in his left ear following working with loud outdoor machinery without ear protection for few hours. He described his tinnitus as a constant mix of white noise and hissing. Occasionally he heard a high-pitched buzzing (lasts 3-4 minutes) in addition to his constant tinnitus. Tinnitus seemed to have become louder recently due to the pressures related to COVID-19 lockdown and the experience of COVID-19 infection in April 2020. Only occasionally tinnitus was perceived in his right ear too. He was under ENT & Audiology colleagues with regard to his hearing rehabilitation and TMJ treatment as well as psychology colleagues for depression and anxiety.
I have provided 14 sessions of specialist rehabilitative programme on tinnitus management based on cognitive behavioural therapy (CBT) approach via video (from distance)1-5. The change in tinnitus loudness, effect of tinnitus on life, insomnia and depression as measured via Visual Analogue Scale6, Tinnitus Handicap Inventory7, Insomnia Severity Index8 and the PHQ-99, respectively, are shown in the graph below:
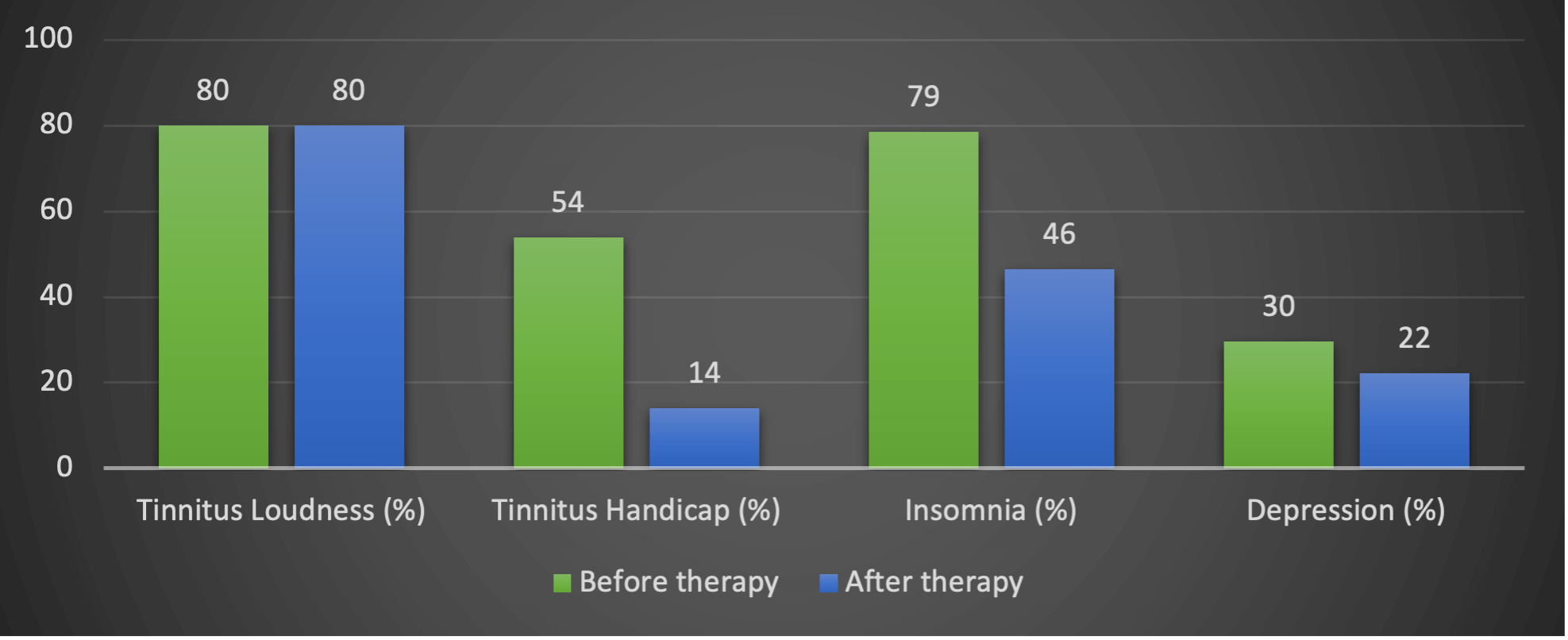 As shown in the graph, there seems to be considerable improvements in his ability to manage his tinnitus. The impact of tinnitus on his sleep has also been reduced. No significant change in self-report tinnitus loudness as expected. This shows although tinnitus remained unchanged he became more confident in managing it, the exact aim of the treatment.
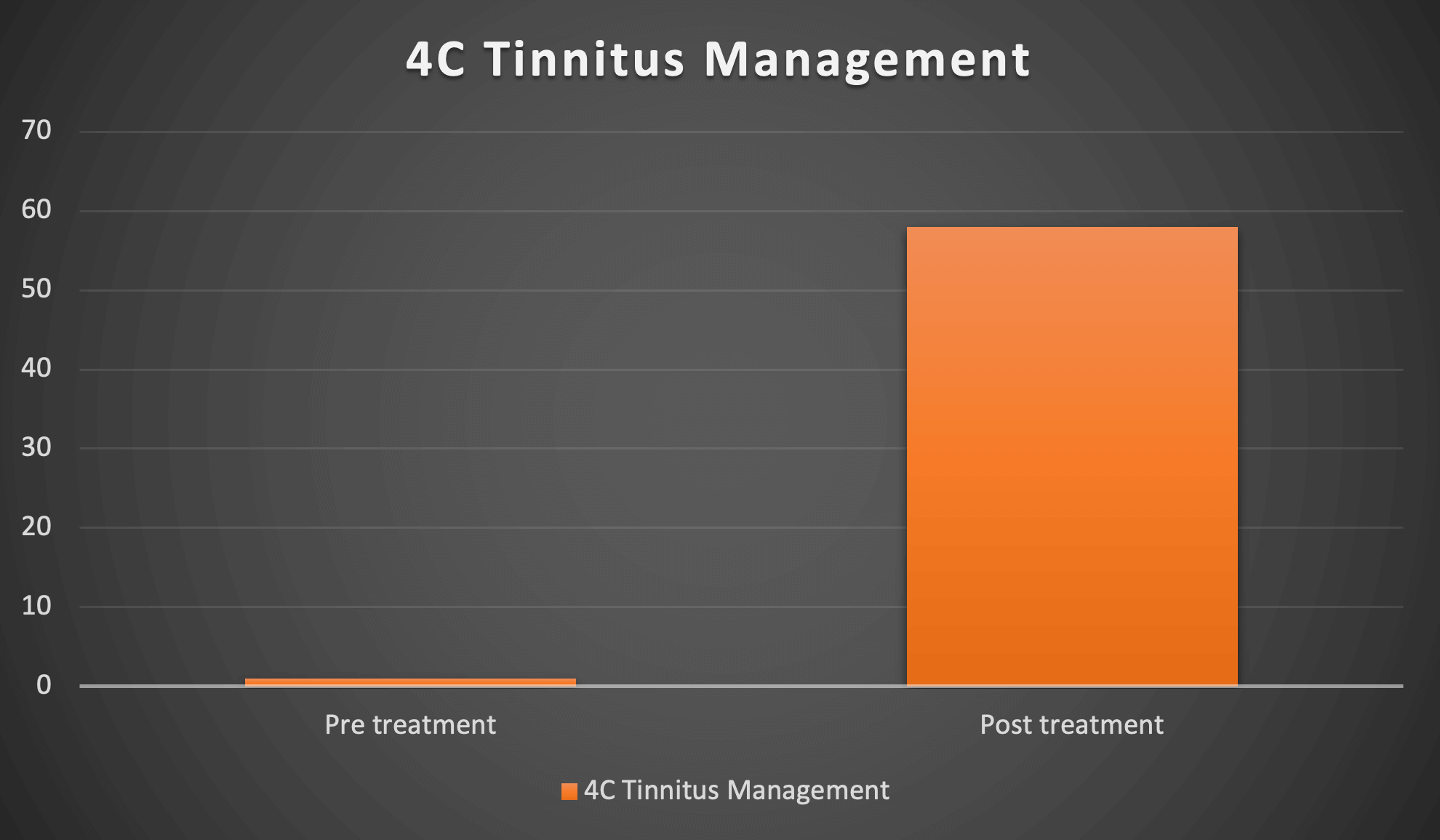
As illustrated in the graph below his score on 4C Tinnitus Management Questionnaire improved from 0% to 54%. The lowest possible score is 0% which means not confident at all in managing tinnitus. The highest possible score is 100% which means confident in managing this condition.
As shown in the graph, there seems to be considerable improvements in his ability to manage his tinnitus. The impact of tinnitus on his sleep has also been reduced. No significant change in self-report tinnitus loudness as expected. This shows although tinnitus remained unchanged he became more confident in managing it, the exact aim of the treatment.
As illustrated in the graph below his score on 4C Tinnitus Management Questionnaire improved from 0% to 54%. The lowest possible score is 0% which means not confident at all in managing tinnitus. The highest possible score is 100% which means confident in managing this condition.
 In addition, his scores on self-report screening questionnaires for psychological disorders were within the normal range.
In addition, his scores on self-report screening questionnaires for psychological disorders were within the normal range.
Conclusion
David has complied with the treatments provided and made considerable improvement in managing his tinnitus.
Feedback from the patient
Hashir has an excellent understanding and obviously a deep well of experience in treating various different tinnitus sufferers. He is empathetic and realistically understands the difficulty that tinnitus causes people day to day and the effects it has on any given persons psychology. He is always positive and warming in his nature and this shows through whilst data gathering and talking about potentially sensitive issues. His treatment programme is very thorough and leaves no stone unturned in trying to get to the bottom of how one may feel about tinnitus and what your thoughts are. He has taught me to change the way that I think about tinnitus, be more positive and get on with life in a more productive way. I would highly recommend Hashir for tinnitus treatment through the use of CBT and its associated benefits.
References
- Aazh H, Allott R. Cognitive behavioural therapy in management of hyperacusis: a narrative review and clinical implementation. Auditory and Vestibular Research 2016;25:63-74.
- Aazh H, Bryant C, Moore BCJ. Patients’ perspectives about the acceptability and effectiveness of audiologist-delivered cognitive behavioral therapy for tinnitus and/or hyperacusis rehabilitation. American Journal of Audiology 2020;28:973-985.
- Aazh H, Landgrebe M, Danesh A et al. Cognitive behavioral therapy for alleviating the distress caused by tinnitus, hyperacusis and misophonia: Current perspectives. Psychology Research and Behavior Management 2019;23:991-1002.
- Aazh H, Moore BCJ. Proportion and characteristics of patients who were offered, enrolled in and completed audiologist-delivered cognitive behavioural therapy for tinnitus and hyperacusis rehabilitation in a specialist UK clinic. International Journal of Audiology 2018;57:415-425.
- Aazh H, Moore BCJ. Effectiveness of audiologist-delivered cognitive behavioral therapy for tinnitus and hyperacusis rehabilitation: outcomes for patients treated in routine practice American Journal of Audiology 2018;27:547-558.
- Adamchic I, Langguth B, Hauptmann C et al. Psychometric evaluation of visual analog scale for the assessment of chronic tinnitus. . American Journal of Audiology 2012;21:215-225.
- Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol 1998;9:153-60.
- Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine 2001;2:297-307.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13.